A new study published online ahead of print in the International Journal of Hygiene and Environmental Health is one of the first to examine levels of chemicals in the ambient air of a real-life setting in the presence of electronic cigarette use.
(See: Schober W, et al. Use of electronic cigarettes [e-cigarettes] impairs indoor air quality and increase FeNO levels of e-cigarette consumers. International Journal of Hygiene and Environmental Health 2013; doie: 10.1016/j.ijheh.2013.11.003.)
The study analyzed the levels of a large number of pollutants in the ambient air of a room in an office building during the presence of three smokers using electronic cigarettes. The room was moderately ventilated at 0.56 air changes per hour.
The most important results were as follows:
1. "Indoor concentrations of CO and CO2 showed no difference between control and vaping periods."
2. "Formaldehyde, benzene and the pyrolysis products acrolein and acetone did not exceed background concentrations."
3. "With regard to the seven PAH classified as probable carcinogens by the IARC, the concentrations increased on average by 20% from 122.8 ng/m3 (control) to 147.3 + 26.2 ng/m3."
4. "No significant increase was observed for the toxic and potentially carcinogenic elements cadmium, arsenic and thallium."
5. "The concentrations of elements and metals showed a 2.4-fold increase for aluminum." [However, there was no significant increase for any other metal, including copper, chromium, nickel, lead, tin, vanadium, or zinc.]
The Rest of the Story
This study, although limited to only three brands of electronic cigarettes, provides reassuring evidence that there do not, at present, appear to be major concerns about substantial health hazards associated with secondhand exposure to electronic cigarettes.
Prior to this study, the most significant health concern regarding passive vaping was the possibility of exposure to carcinogenic and toxic aldehydes and pyrolysis products including formaldehyde, acrolein, and acetone. However, this study found no increase in concentrations of any of these pollutants under realistic (real-life) conditions.
Despite a small increase in polycyclic aromatic hydrocarbon concentrations, there were no significant increases for any of the known or probably carcinogenic compounds.
With the exception of aluminum, the concentrations of most metals were substantially lower during vaping than in the no vaping condition. Metals therefore do not appear to be a significant health issue at this point in time.
In summary, this study helps to alleviate concerns raised by prior research and does not raise any new concerns. While more research is clearly needed, especially because there are so many different brands of electronic cigarettes on the market, the current evidence does not point to any substantial health hazards associated with passive vaping.
In light of these findings, the best that the study authors could do to implicate electronic cigarettes as a human health hazard was to proclaim that "e-cigarettes are not emission-free." If that is the worst thing that thsee researchers can say, then it certainly doesn't appear to rise to the level of a known health hazard for which government intervention is necessary at this time.
There are clearly two ways to spin this study. One is to emphasize the study's reassuring findings that there were no substantial causes for serious concern. Another is to spin it as these authors did, stating their conclusion as follows:
"Analysis of indoor air quality during vaping sessions showed that e-cigarettes are not emission-free." This was the second time the authors used this phrasing to summarize their findings. Right now, that e-cigarettes are not emission free appears to be about the most alarming thing that can be said about them.
Thursday, January 30, 2014
Wednesday, January 29, 2014
NEJM Commentary Written by Anti-Tobacco Researchers Hides Conflicts of Interest with Big Pharma
An article published last week in the New England Journal of Medicine discusses strategies for reducing smoking, including the use of pharmaceutical products such as nicotine replacement therapy and other drugs. The article argues that every patient who wishes to quit should be provided with smoking cessation drugs, as opposed to relying upon other approaches, such as counseling or cold turkey quitting.
Because the advice given to physicians in this column conflicts with scientific evidence and undermines the principle of physician autonomy, readers may naturally be curious whether the authors of this commentary have any history of financial conflicts of interest with pharmaceutical companies that products the products discussed in the article.
Fortunately, readers can be rest assured that there were no relevant conflicts to disclose. All three of the co-authors - Dr. Michael Fiore, Dr. Steven Schroeder, and Dr. Timothy Baker - completed disclosure forms indicating that they have nothing to disclose, which implies that there is no relevant history of financial relationships of any of these authors with pharmaceutical companies.
Specifically, in completing section 5 of the form, each of the authors proclaimed that there were: "No other relationships/conditions/circumstances that present a potential conflict of interest." This section refers to financial interests that were not disclosed earlier in the form. The disclosures earlier in the form relate to financial interests present during the past 36 months. Importantly, however, the additional disclosures in section 5 do not have any stated time frame. The directions indicate that authors must "use this section to report other relationships or activities that readers could perceive to have influenced, or that give the appearance of potentially influencing, what you wrote in the submitted work."
Since all three authors indicated in section 5 that there are no other relationships or activities that readers could perceive to have influenced their work, we can conclude that none of these authors has any significant history of financial relationships with Big Pharma.
The Rest of the Story
The rest of the story is that two of the three authors are hiding relevant financial conflicts of interest with Big Pharma that I believe should have been disclosed in the paper.
Dr. Fiore
The truth is that Dr. Fiore actually has a long history of significant financial relationships with pharmaceutical companies that manufacture smoking cessation drugs, none of which are acknowledged in his disclosure. Here is what is being hidden from readers:
1. According to his own 2008 JAMA article: "In the past 5 years, Dr Fiore reports that he has lectured and consulted for Pfizer and has served as an investigator on research studies at the University of Wisconsin (UW) that were supported by GlaxoSmithKline, Nabi, Pfizer, and sanofi-aventis."
2. According to his own sworn testimony, at the time of his chairing in 2008 of an expert NIH panel to make recommendations about the recommended clinical strategies for promoting smoking cessation, Dr. Fiore received up to $50,000 in annual resources from GlaxoSmithKline to support his educational, research, and policy activities.
3. In 2006, Dr. Fiore acknowledged that "I have done some consulting work for pharmaceutical companies over the years. Over the past five years, my outside consulting work on an annual basis has ranged between about $10,000 and $30,000 or $40,000 per year."
4. In 1998, the University of Wisconsin appointed him to a named chair, made possible by an unrestricted gift to the University from GlaxoWellcome.
5. In the past, "Dr. Fiore has served as a consultant for, given lectures sponsored by, or has conducted research sponsored by Ciba-Geigy, SmithKline Beecham, Lederle Laboratories, McNeil Consumer Products, Elan Pharmaceutical, Pharmacia, and Glaxo Wellcome."
6. Dr. Fiore directs a tobacco research center that received nearly $1 million in funding from makers of quit-smoking medicine in 2004 and $400,000 in 2005.
7. In a recent set of two articles on treatment for smoking cessation published in the Annals of Behavioral Medicine in April 2011 (article 1; article 2), the conflict of interest statement regarding Dr. Fiore acknowledges that: "Over the last 3 years, Michael C. Fiore served as an investigator on research studies at the University of Wisconsin that were funded by Nabi Biopharmaceuticals."
8. In a December 2010 article on treatment for smoking cessation published in the Wisconsin Medical Journal, the conflict of interest statement regarding Dr. Fiore acknowledges that: "Over the last 3 years, Dr Fiore has served as an investigator in research studies at the University of Wisconsin that were funded by Pfizer and Nabi Biopharmaceuticals."
Amazingly, none of these conflicts of interest are reported in the paper and the reader has no way of knowing this long history of financial conflicts of interest with Big Pharma. I imagine that most readers would be shocked to find out about this intense and long history of financial conflict with Big Pharma, given that Dr. Fiore reported no conflicts of interest.
Dr. Baker
The truth is that Dr. Baker also has a long and significant history of financial relationships with pharmaceutical companies that manufacture smoking cessation drugs. Here is what is being hidden from readers:
1. In 2008, Dr. Baker reported that: "he has served as a co-investigator on research studies at the University of Wisconsin that were sponsored by four pharmaceutical companies."
2. In 2000, Dr. Baker disclosed as follows: "Timothy Baker has served as a consultant for, given lectures sponsored by, or has conducted research sponsored by Elan Pharmaceutical, SmithKline Beecham, Glaxo Wellcome, and Lederle."
3. As recently as 2012, Dr. Baker disclosed in an article that his research involved financial support from GlaxoSmithKline in the form of free medication provided to study participants.
4. In another 2012 paper, Dr. Baker also acknowledged that GlaxoSmithKline provided financial support in the form of free study medication. The same disclosure was made in another 2012 paper. And in another paper as well.
5. According to a 2011 paper: "Timothy B. Baker has served as a consultant, given lectures sponsored by, or has conducted research sponsored by GlaxoSmithKline, Nabi Biopharmaceuticals, Pfizer, and Sanofi-Synthelabo."
6. In a 2010 paper, Dr. Baker acknowledged "research grants from Pfizer, GlaxoSmithKline, Nabi Biopharmaceuticals, and Sanofi."That paper itself involved research with financial support from GlaxoSmithKline in the form of free study medication.
Again, amazingly, none of these conflicts of interest are reported in the paper and the reader has no way of knowing this long history of financial conflicts of interest with Big Pharma.
Here, not only does it appear that Dr. Baker has failed to disclose conflicts that should have been revealed in section 5 of the form, but I have to question whether he has also hidden information that should have been disclosed in section 3. The instructions to that section clearly indicate that research involving drugs provided by pharmaceutical companies is to be included in this section. Since the research was ongoing in 2012 (that is the year in which papers were continuing to be published), it appears to me that this financial conflict falls within the 36 month period about which the form inquires.
Either way, Dr. Baker's participation in research that was financiallly supported by GlaxoSmithKline should have been reported in his disclosure.
3. Dr. Schroeder
Dr. Schroeder is the only one of the three authors who does not appear to be hiding a significant financial ionflict of interest. However, it is worth noting that Dr. Schroeder's center lists Pfizer as a partner. It is not clear to me what this means. If Pfizer is a financial partner, then this should have been disclosed in the article. But even if Pfizer is just a partner in terms of working together on a project, I would still view that as a conflict of interest that should have been disclosed.
Summary
For years, we in tobacco control have attacked tobacco industry-funded scientists or researchers who consulted for tobacco companies for not disclosing their conflicts of interest. It is therefore quite unfortunate, and ironic, that tobacco control researchers do not appear to take their own conflicts of interest seriously and that they, too, are hiding these conflicts from the public.
As I previously articulated, the hiding of these conflicts of interest damages public health in four ways:
Because the advice given to physicians in this column conflicts with scientific evidence and undermines the principle of physician autonomy, readers may naturally be curious whether the authors of this commentary have any history of financial conflicts of interest with pharmaceutical companies that products the products discussed in the article.
Fortunately, readers can be rest assured that there were no relevant conflicts to disclose. All three of the co-authors - Dr. Michael Fiore, Dr. Steven Schroeder, and Dr. Timothy Baker - completed disclosure forms indicating that they have nothing to disclose, which implies that there is no relevant history of financial relationships of any of these authors with pharmaceutical companies.
Specifically, in completing section 5 of the form, each of the authors proclaimed that there were: "No other relationships/conditions/circumstances that present a potential conflict of interest." This section refers to financial interests that were not disclosed earlier in the form. The disclosures earlier in the form relate to financial interests present during the past 36 months. Importantly, however, the additional disclosures in section 5 do not have any stated time frame. The directions indicate that authors must "use this section to report other relationships or activities that readers could perceive to have influenced, or that give the appearance of potentially influencing, what you wrote in the submitted work."
Since all three authors indicated in section 5 that there are no other relationships or activities that readers could perceive to have influenced their work, we can conclude that none of these authors has any significant history of financial relationships with Big Pharma.
The Rest of the Story
The rest of the story is that two of the three authors are hiding relevant financial conflicts of interest with Big Pharma that I believe should have been disclosed in the paper.
Dr. Fiore
The truth is that Dr. Fiore actually has a long history of significant financial relationships with pharmaceutical companies that manufacture smoking cessation drugs, none of which are acknowledged in his disclosure. Here is what is being hidden from readers:
1. According to his own 2008 JAMA article: "In the past 5 years, Dr Fiore reports that he has lectured and consulted for Pfizer and has served as an investigator on research studies at the University of Wisconsin (UW) that were supported by GlaxoSmithKline, Nabi, Pfizer, and sanofi-aventis."
2. According to his own sworn testimony, at the time of his chairing in 2008 of an expert NIH panel to make recommendations about the recommended clinical strategies for promoting smoking cessation, Dr. Fiore received up to $50,000 in annual resources from GlaxoSmithKline to support his educational, research, and policy activities.
3. In 2006, Dr. Fiore acknowledged that "I have done some consulting work for pharmaceutical companies over the years. Over the past five years, my outside consulting work on an annual basis has ranged between about $10,000 and $30,000 or $40,000 per year."
4. In 1998, the University of Wisconsin appointed him to a named chair, made possible by an unrestricted gift to the University from GlaxoWellcome.
5. In the past, "Dr. Fiore has served as a consultant for, given lectures sponsored by, or has conducted research sponsored by Ciba-Geigy, SmithKline Beecham, Lederle Laboratories, McNeil Consumer Products, Elan Pharmaceutical, Pharmacia, and Glaxo Wellcome."
6. Dr. Fiore directs a tobacco research center that received nearly $1 million in funding from makers of quit-smoking medicine in 2004 and $400,000 in 2005.
7. In a recent set of two articles on treatment for smoking cessation published in the Annals of Behavioral Medicine in April 2011 (article 1; article 2), the conflict of interest statement regarding Dr. Fiore acknowledges that: "Over the last 3 years, Michael C. Fiore served as an investigator on research studies at the University of Wisconsin that were funded by Nabi Biopharmaceuticals."
8. In a December 2010 article on treatment for smoking cessation published in the Wisconsin Medical Journal, the conflict of interest statement regarding Dr. Fiore acknowledges that: "Over the last 3 years, Dr Fiore has served as an investigator in research studies at the University of Wisconsin that were funded by Pfizer and Nabi Biopharmaceuticals."
Amazingly, none of these conflicts of interest are reported in the paper and the reader has no way of knowing this long history of financial conflicts of interest with Big Pharma. I imagine that most readers would be shocked to find out about this intense and long history of financial conflict with Big Pharma, given that Dr. Fiore reported no conflicts of interest.
Dr. Baker
The truth is that Dr. Baker also has a long and significant history of financial relationships with pharmaceutical companies that manufacture smoking cessation drugs. Here is what is being hidden from readers:
1. In 2008, Dr. Baker reported that: "he has served as a co-investigator on research studies at the University of Wisconsin that were sponsored by four pharmaceutical companies."
2. In 2000, Dr. Baker disclosed as follows: "Timothy Baker has served as a consultant for, given lectures sponsored by, or has conducted research sponsored by Elan Pharmaceutical, SmithKline Beecham, Glaxo Wellcome, and Lederle."
3. As recently as 2012, Dr. Baker disclosed in an article that his research involved financial support from GlaxoSmithKline in the form of free medication provided to study participants.
4. In another 2012 paper, Dr. Baker also acknowledged that GlaxoSmithKline provided financial support in the form of free study medication. The same disclosure was made in another 2012 paper. And in another paper as well.
5. According to a 2011 paper: "Timothy B. Baker has served as a consultant, given lectures sponsored by, or has conducted research sponsored by GlaxoSmithKline, Nabi Biopharmaceuticals, Pfizer, and Sanofi-Synthelabo."
6. In a 2010 paper, Dr. Baker acknowledged "research grants from Pfizer, GlaxoSmithKline, Nabi Biopharmaceuticals, and Sanofi."That paper itself involved research with financial support from GlaxoSmithKline in the form of free study medication.
Again, amazingly, none of these conflicts of interest are reported in the paper and the reader has no way of knowing this long history of financial conflicts of interest with Big Pharma.
Here, not only does it appear that Dr. Baker has failed to disclose conflicts that should have been revealed in section 5 of the form, but I have to question whether he has also hidden information that should have been disclosed in section 3. The instructions to that section clearly indicate that research involving drugs provided by pharmaceutical companies is to be included in this section. Since the research was ongoing in 2012 (that is the year in which papers were continuing to be published), it appears to me that this financial conflict falls within the 36 month period about which the form inquires.
Either way, Dr. Baker's participation in research that was financiallly supported by GlaxoSmithKline should have been reported in his disclosure.
3. Dr. Schroeder
Dr. Schroeder is the only one of the three authors who does not appear to be hiding a significant financial ionflict of interest. However, it is worth noting that Dr. Schroeder's center lists Pfizer as a partner. It is not clear to me what this means. If Pfizer is a financial partner, then this should have been disclosed in the article. But even if Pfizer is just a partner in terms of working together on a project, I would still view that as a conflict of interest that should have been disclosed.
Summary
For years, we in tobacco control have attacked tobacco industry-funded scientists or researchers who consulted for tobacco companies for not disclosing their conflicts of interest. It is therefore quite unfortunate, and ironic, that tobacco control researchers do not appear to take their own conflicts of interest seriously and that they, too, are hiding these conflicts from the public.
As I previously articulated, the hiding of these conflicts of interest damages public health in four ways:
- It violates public health ethics and could be damaging to the entire field of tobacco control;
- It degrades the research integrity of tobacco control;
- It makes us hypocrites when we criticize failed tobacco industry disclosures; and
- It hides the influence of Big Pharma money on the field of tobacco control and hinders smoking cessation efforts.
Tuesday, January 28, 2014
Luther Terry Remembered as Surgeon General Who Released 1964 Smoking Report, But There's More to His Legacy
As tobacco control advocates commemorate the 50th anniversary of the release of the 1964 Surgeon General's report on smoking by Dr. Luther Terry, we are praising Dr. Terry for his groundbreaking and pivotal work that many view as having started the tobacco control movement. Dr. Terry served as Surgeon General of the United States Public Health Service from 1961 to 1965.
In fact, the American Cancer Society (ACS) has established a series of awards given in Dr. Terry's honor and memory. According to the ACS: "The Luther L. Terry Awards are presented triennially and in conjunction with the World Conference on Tobacco OR Health. These awards recognize outstanding worldwide achievement in the field of tobacco control. Awards are presented in six categories: Outstanding Individual Leadership, Outstanding Organization, Outstanding Research Contribution, Exemplary Leadership by a Government Ministry, Distinguished Career, and Outstanding Community Service. Named for the late United States Surgeon General Luther L. Terry, M.D., whose groundbreaking work established the foundation for public health scrutiny of the dangers of tobacco use, the Awards honor outstanding leadership and accomplishment, are synonymous with excellence, and signify that the recipients are among the very best in the world at what they do."
The Rest of the Story
Sadly, there is more to the story of Dr. Luther Terry's reign as Surgeon General and more to the legacy of his having served this critical role as leader of the Public Health Service.
Between 1961 and 1965 - during the entire time that Dr. Terry was heading the Public Health Service as Surgeon General - the Service was conducting an unethical and racist study in which it denied antibiotic treatment to African American men with advanced syphilis in order to observe the debilitating and fatal long-term sequelae of this essentially 100% treatable infection.
At the time the experiment was initiated in 1932, the treatment for syphilis involved toxic drugs. However, by the 1940's, penicillin was readily available as a treatment for this infection. Nevertheless, the study continued and penicillin was not made available to these black men. Nor were they informed about the availability of the medicine or even of what disease they actually had.
Shockingly, no one stopped the experiment. That includes Luther Terry. The rest of the story is that Dr. Terry, who presided over the Tuskegee Experiment from 1961 to 1965, failed to stop the study, even though penicillin had been available for the past 20 years.
And Dr. Terry failed to stop the study in 1965, even after the 1964 World Health Organization's Helsinki Declaration clearly articulated the ethical imperative of informed consent for human medical experimentation.
Along with the Surgeon General's who served before him, Dr. Terry shares in the culpability for the 128 deaths and 19 cases of congenital syphilis that were caused by the government's irresponsibility and racism. While it is not pretty, these are the facts and we cannot simply ignore this atrocity and pretend that it is not part of Dr. Terry's legacy.
Personally, I cannot condone the idea of establishing an award in Dr. Terry's name, and I would hope that the American Cancer Society would rename its award so as not to commemorate the legacy of a physician who - during his tenure as a government leader - directed one of the worst, most unethical, and most racist medical and public health atrocities of our time.
We certainly should not forget Dr. Terry's amazing work in bringing the issue of the health effects of smoking to public light. But at the same time, we must not forget his responsibility in the atrocity that is the Tuskegee study.
In fact, the American Cancer Society (ACS) has established a series of awards given in Dr. Terry's honor and memory. According to the ACS: "The Luther L. Terry Awards are presented triennially and in conjunction with the World Conference on Tobacco OR Health. These awards recognize outstanding worldwide achievement in the field of tobacco control. Awards are presented in six categories: Outstanding Individual Leadership, Outstanding Organization, Outstanding Research Contribution, Exemplary Leadership by a Government Ministry, Distinguished Career, and Outstanding Community Service. Named for the late United States Surgeon General Luther L. Terry, M.D., whose groundbreaking work established the foundation for public health scrutiny of the dangers of tobacco use, the Awards honor outstanding leadership and accomplishment, are synonymous with excellence, and signify that the recipients are among the very best in the world at what they do."
The Rest of the Story
Sadly, there is more to the story of Dr. Luther Terry's reign as Surgeon General and more to the legacy of his having served this critical role as leader of the Public Health Service.
Between 1961 and 1965 - during the entire time that Dr. Terry was heading the Public Health Service as Surgeon General - the Service was conducting an unethical and racist study in which it denied antibiotic treatment to African American men with advanced syphilis in order to observe the debilitating and fatal long-term sequelae of this essentially 100% treatable infection.
At the time the experiment was initiated in 1932, the treatment for syphilis involved toxic drugs. However, by the 1940's, penicillin was readily available as a treatment for this infection. Nevertheless, the study continued and penicillin was not made available to these black men. Nor were they informed about the availability of the medicine or even of what disease they actually had.
Shockingly, no one stopped the experiment. That includes Luther Terry. The rest of the story is that Dr. Terry, who presided over the Tuskegee Experiment from 1961 to 1965, failed to stop the study, even though penicillin had been available for the past 20 years.
And Dr. Terry failed to stop the study in 1965, even after the 1964 World Health Organization's Helsinki Declaration clearly articulated the ethical imperative of informed consent for human medical experimentation.
Along with the Surgeon General's who served before him, Dr. Terry shares in the culpability for the 128 deaths and 19 cases of congenital syphilis that were caused by the government's irresponsibility and racism. While it is not pretty, these are the facts and we cannot simply ignore this atrocity and pretend that it is not part of Dr. Terry's legacy.
Personally, I cannot condone the idea of establishing an award in Dr. Terry's name, and I would hope that the American Cancer Society would rename its award so as not to commemorate the legacy of a physician who - during his tenure as a government leader - directed one of the worst, most unethical, and most racist medical and public health atrocities of our time.
We certainly should not forget Dr. Terry's amazing work in bringing the issue of the health effects of smoking to public light. But at the same time, we must not forget his responsibility in the atrocity that is the Tuskegee study.
Monday, January 27, 2014
Rest of the Story Author Takes it Under the Chin for Suggesting that Filtered Cigarettes Pose Slightly Lower Lung Cancer Risk
Once again, I was attacked by my colleagues, including two co-authors of the 2014 Surgeon General's report, for having the nerve to suggest that lifelong smokers of filtered cigarettes may have slightly lower lung cancer risk than lifetime smokers of non-filtered cigarettes.
Remember that I did not argue that a smoker switching from a non-filtered to a filtered cigarette brand will reduce her cancer risk. It may be that vigorous compensation offsets the impact of such a change. However, I do believe that the scientific evidence supports the contention that all else being equal, a lifelong smoker of non-filtered cigarettes faces a slightly higher cancer risk than a lifelong smoker of filtered cigarettes.
While the attacks were mostly personal, and not worthy of expounding here, the shred of substance was that more recent studies which compared lung cancer risks of successive cohorts of smokers have found increased risk among more recent cohorts. From these studies, the Surgeon General's report - and these co-authors - conclude that filters must convey an increased risk of cancer.
This argument is fallacious, I believe, because there are many things that changed from one cohort to the next. The introduction of cigarette filters is only one such change. To assume that any observed changes in cancer risk from one cohort to the next must be attributable to one particular change - the filter - is not appropriate, in my view.
Instead, I think that studies which specifically compare lung cancer risk between lifelong smokers of filtered vs. non-filtered cigarettes during the same time period are most informative regarding the relative cancer risks of these products. And multiple studies along these lines, including recent studies, have reported a slightly decreased risk associated with lifetime smoking of filtered vs. non-filtered cigarettes.
These studies are simply ignored by the Surgeon General's report and by my colleagues who have attacked me. It would be one thing if there were no evidence for my opinions, but it's hardly appropriate to attack an individual for expressing an opinion that is backed up by scientific studies.
This issue is particularly important because based on the arguments of these authors, the FDA should ban filtered cigarettes in order to protect the public's health. But in my opinion, such a move could be disastrous because it would result in a dramatic increase in tar delivery and possibly carcinogen dose, potentially leading to an increase, rather than a decrease in cancer.
The Rest of the Story
What is most disturbing to me about this story is that there is clearly no room for a difference in opinion in the tobacco control movement about certain dogmatic elements of the field. You can't express disagreement without facing personal attack, no matter how well you support your argument with scientific evidence. Like a religion, you can't challenge the gospel-like nature of movement's mantra without being viewed as a heretic.
Fortunately, I'm used to this treatment, so I'm not going to be bullied into backing down. I believe that a lot is at stake here, because a wrong move on the part of the FDA in banning filtered cigarettes could literally lead to an increase in cigarette-related deaths.
Remember that I did not argue that a smoker switching from a non-filtered to a filtered cigarette brand will reduce her cancer risk. It may be that vigorous compensation offsets the impact of such a change. However, I do believe that the scientific evidence supports the contention that all else being equal, a lifelong smoker of non-filtered cigarettes faces a slightly higher cancer risk than a lifelong smoker of filtered cigarettes.
While the attacks were mostly personal, and not worthy of expounding here, the shred of substance was that more recent studies which compared lung cancer risks of successive cohorts of smokers have found increased risk among more recent cohorts. From these studies, the Surgeon General's report - and these co-authors - conclude that filters must convey an increased risk of cancer.
This argument is fallacious, I believe, because there are many things that changed from one cohort to the next. The introduction of cigarette filters is only one such change. To assume that any observed changes in cancer risk from one cohort to the next must be attributable to one particular change - the filter - is not appropriate, in my view.
Instead, I think that studies which specifically compare lung cancer risk between lifelong smokers of filtered vs. non-filtered cigarettes during the same time period are most informative regarding the relative cancer risks of these products. And multiple studies along these lines, including recent studies, have reported a slightly decreased risk associated with lifetime smoking of filtered vs. non-filtered cigarettes.
These studies are simply ignored by the Surgeon General's report and by my colleagues who have attacked me. It would be one thing if there were no evidence for my opinions, but it's hardly appropriate to attack an individual for expressing an opinion that is backed up by scientific studies.
This issue is particularly important because based on the arguments of these authors, the FDA should ban filtered cigarettes in order to protect the public's health. But in my opinion, such a move could be disastrous because it would result in a dramatic increase in tar delivery and possibly carcinogen dose, potentially leading to an increase, rather than a decrease in cancer.
The Rest of the Story
What is most disturbing to me about this story is that there is clearly no room for a difference in opinion in the tobacco control movement about certain dogmatic elements of the field. You can't express disagreement without facing personal attack, no matter how well you support your argument with scientific evidence. Like a religion, you can't challenge the gospel-like nature of movement's mantra without being viewed as a heretic.
Fortunately, I'm used to this treatment, so I'm not going to be bullied into backing down. I believe that a lot is at stake here, because a wrong move on the part of the FDA in banning filtered cigarettes could literally lead to an increase in cigarette-related deaths.
Surgeon General's Report Implicates Filtered Cigarettes in Increasing Cancer Risk
According to an article at Law360.com, the recently-released Surgeon General's report's conclusion that cigarette filters may actually increase the risk of lung cancer could lead to a new wave of class-action lawsuits against cigarette companies.
According to the article: "The U.S. surgeon general's landmark finding last week that filtered cigarettes may actually increase the risk of lung cancer could lead to a flurry of new lawsuits against tobacco companies and even expand cigarette litigation outside of Florida, where it has flourished for nearly a decade."
The Surgeon General's report concludes that: "The introduction of ventilated filters, or changes in the design and composition of cigarettes that accompanied their introduction, may have increased the carcinogenicity of cigarette smoke."
The introduction and proliferation of filtered cigarettes occurred mostly in the decades preceding and following the 1964 Surgeon General's report and was mostly complete by 1974. Further reductions in tar yield occurred through other mechanisms, as by 1974, most cigarette brands were filtered.
The Rest of the Story
While it is undeniably true that subsequent changes to the tar yield of cigarettes (changes subsequent to the introduction of filters) did not lower the lung cancer risk associated with cigarette smoking, one must be careful in concluding that the introduction of the filter resulted in an increase in lung cancer risk.
In fact, the bulk of the evidence suggests that the introduction of the cigarette filter, while obviously not making cigarettes substantially safer, did result in small but measurable declines in cancer risk. These declines occurred due to a tremendous reduction in tar yield, from levels as high as 40-50 mg down to less than 20 mg. The evidence suggests that further declines - to levels below this massive initial drop - were not associated with further declines in cancer risk.
Thus, it appears that cigarette filters did produce a small but measurable decline in cancer risks associated with smoking, while further design changes that lowered tar levels did not. In other words, there is evidence that filtered cigarettes produce lower cancer risks than non-filtered cigarettes. However, within the filtered cigarette category, there is no evidence that low-tar cigarettes confer any reduced cancer risk.
Unfortunately, the Surgeon General's report conflated these two types of changes and as a result, its conclusion that the introduction of the filter actually increased cancer risk is inaccurate and in conflict with the scientific evidence.
One of my first assignments at the Office on Smoking and Health at CDC was to evaluate the evidence regarding the relationship between changes in tar yield of cigarettes and the risk of lung cancer. I examined the literature regarding both the introduction of the filter and other design changes that subsequently led to very low tar yields. My conclusion was that the filter itself produced a massive decline in tar yields, so great that even with smoker compensation, the lung cancer risk declined. However, further declines in tar yields were apparently not sufficient to overcome compensation, and lung cancer risks did not decline any further. Thus, my conclusion was that the filter produced small but measurable declines in lung cancer risk, but low-tar cigarettes within the filtered cigarette category conveyed no decrease in lung cancer risk.
The scientific literature supporting the conclusion that filtered cigarettes are associated with a lower cancer risk than non-filtered cigarettes is substantial. I will not present the entire literature, but here are some representative studies:
Harris et al., in perhaps the most comprehensive and definitive study on this issue, found a clear increase in cancer risk associated with non-filtered cigarettes. As they reported: "Compared with smokers of medium tar (15-21 mg) filter cigarettes, risk was higher among men and women who smoked high tar (> or = 22 mg) non-filter brands (hazard ratio 1.44, 95% confidence interval 1.20 to 1.73, and 1.64, 1.26 to 2.15, respectively)."
Pogoda et al. found that the risk of acute myeloid leukemia is significantly higher among smokers of non-filtered compared to filtered cigarettes: "Odds ratios were significantly increased for ... subjects who smoked ... nonfiltered products (OR = 2.3, 95 percent CI: 1.1, 4.9)."
Sidney et al. found that among women, lung cancer risk was lower for lifelong smokers of filtered cigarettes than smokers of non-filtered cigarettes: "in long-term (> 20 years) smokers, the risk of lung cancer was decreased in women who had smoked filtered cigarettes for 20 or more years relative to lifelong smokers of unfiltered cigarettes (RR = 0.36, CI = 0.18-0.75)."
Falk et al., in a study of the risk for laryngeal cancer, found that: "Higher risks were associated with smoking nonfiltered than filtered cigarettes." For those who smoked filtered cigarettes, the OR was 5.9 (95% CI = 2.4-14.4); for those who smoked non-filtered cigarettes, the OR was 9.0 (95% CI = 3.2-25.1).
Luchtenborg et al. found that while non-filtered cigarettes increased the risk for colon cancer (OR 1.59; 95% CI, 1.15-2.21; P(trend) = 0.001), filtered cigarettes did not increase colon cancer risk (OR 1.05; 95% CI, 0.79-1.39; P(trend) = 0.98).
Wynder et al. reported slightly lower bladder cancer risk among filtered cigarette smokers: "Smokers of filtered cigarettes had a slightly reduced risk of bladder cancer relative to smokers of nonfiltered cigarettes (odds ratio 0.64, 95% confidence interval 0.38 to 1.10 among male smokers; odds ratio 0.74, 95% confidence interval 0.37 to 1.48 among female smokers)."
Hartge et al. found exactly the same result as Wynder's group: "Our data indicated that people who have only smoked unfiltered cigarettes have higher risks."
Sadly, although the Surgeon General's report draws conclusions about the health impact of filtered cigarettes, it only cites one of these seven studies (the Luchtenborg study). And in citing that study, the report merely notes its finding that smoking increases colon cancer risk. It hides this study's finding that this increased colon cancer risk was only detected among smokers of non-filtered cigarettes!
Why does the Surgeon General's report not review the literature on the cancer risks of filtered vs. non-filtered cigarettes, even though it seems to draw a conclusion about this issue? The only answer I can think of is that the report aimed to draw a particular conclusion, rather than to present the facts in an objective way. Apparently, the report was pre-determined to conclude that all design changes to cigarettes increased their cancer risk. It conflated the filter with other sources of tar yield reductions and at the same time, failed to review studies that examined the relative risk of filtered vs. non-filtered cigarettes.
As a result, the report implies that cigarette filters increase lung cancer risk and opens the way for lawsuits based on this claim, as the Law360.com article suggests.
But the truth is more nuanced. While there is no question that low-tar or "light" cigarettes are not safer, it is not the case that the introduction of filters made cigarettes more carcinogenic. I would not be able to testify in a courtroom that I believe filtered cigarettes are more dangerous than non-filtered cigarettes. Nor would I be able to testify that filtered cigarettes and non-filtered cigarettes pose equivalent cancer risk.
It is important to point out that just because the relative risk of cancer associated with filtered cigarettes is lower than that for non-filtered cigarettes, it does not necessarily follow that switching from a non-filtered to a filtered cigarette will reduce one's health risks. It is possible that smokers who make such a switch will compensate because they are used to higher tar levels. It is possible that the observed reduction in cancer risk only holds for lifelong filtered cigarette smokers, as they do not compensate (they never smoked non-filtered cigarettes). In fact, the scientific evidence supports this contention.
The rest of the story is that in yet another area of tobacco control science, the Surgeon General's report is providing a biased view of the scientific evidence.
According to the article: "The U.S. surgeon general's landmark finding last week that filtered cigarettes may actually increase the risk of lung cancer could lead to a flurry of new lawsuits against tobacco companies and even expand cigarette litigation outside of Florida, where it has flourished for nearly a decade."
The Surgeon General's report concludes that: "The introduction of ventilated filters, or changes in the design and composition of cigarettes that accompanied their introduction, may have increased the carcinogenicity of cigarette smoke."
The introduction and proliferation of filtered cigarettes occurred mostly in the decades preceding and following the 1964 Surgeon General's report and was mostly complete by 1974. Further reductions in tar yield occurred through other mechanisms, as by 1974, most cigarette brands were filtered.
The Rest of the Story
While it is undeniably true that subsequent changes to the tar yield of cigarettes (changes subsequent to the introduction of filters) did not lower the lung cancer risk associated with cigarette smoking, one must be careful in concluding that the introduction of the filter resulted in an increase in lung cancer risk.
In fact, the bulk of the evidence suggests that the introduction of the cigarette filter, while obviously not making cigarettes substantially safer, did result in small but measurable declines in cancer risk. These declines occurred due to a tremendous reduction in tar yield, from levels as high as 40-50 mg down to less than 20 mg. The evidence suggests that further declines - to levels below this massive initial drop - were not associated with further declines in cancer risk.
Thus, it appears that cigarette filters did produce a small but measurable decline in cancer risks associated with smoking, while further design changes that lowered tar levels did not. In other words, there is evidence that filtered cigarettes produce lower cancer risks than non-filtered cigarettes. However, within the filtered cigarette category, there is no evidence that low-tar cigarettes confer any reduced cancer risk.
Unfortunately, the Surgeon General's report conflated these two types of changes and as a result, its conclusion that the introduction of the filter actually increased cancer risk is inaccurate and in conflict with the scientific evidence.
One of my first assignments at the Office on Smoking and Health at CDC was to evaluate the evidence regarding the relationship between changes in tar yield of cigarettes and the risk of lung cancer. I examined the literature regarding both the introduction of the filter and other design changes that subsequently led to very low tar yields. My conclusion was that the filter itself produced a massive decline in tar yields, so great that even with smoker compensation, the lung cancer risk declined. However, further declines in tar yields were apparently not sufficient to overcome compensation, and lung cancer risks did not decline any further. Thus, my conclusion was that the filter produced small but measurable declines in lung cancer risk, but low-tar cigarettes within the filtered cigarette category conveyed no decrease in lung cancer risk.
The scientific literature supporting the conclusion that filtered cigarettes are associated with a lower cancer risk than non-filtered cigarettes is substantial. I will not present the entire literature, but here are some representative studies:
Harris et al., in perhaps the most comprehensive and definitive study on this issue, found a clear increase in cancer risk associated with non-filtered cigarettes. As they reported: "Compared with smokers of medium tar (15-21 mg) filter cigarettes, risk was higher among men and women who smoked high tar (> or = 22 mg) non-filter brands (hazard ratio 1.44, 95% confidence interval 1.20 to 1.73, and 1.64, 1.26 to 2.15, respectively)."
Pogoda et al. found that the risk of acute myeloid leukemia is significantly higher among smokers of non-filtered compared to filtered cigarettes: "Odds ratios were significantly increased for ... subjects who smoked ... nonfiltered products (OR = 2.3, 95 percent CI: 1.1, 4.9)."
Sidney et al. found that among women, lung cancer risk was lower for lifelong smokers of filtered cigarettes than smokers of non-filtered cigarettes: "in long-term (> 20 years) smokers, the risk of lung cancer was decreased in women who had smoked filtered cigarettes for 20 or more years relative to lifelong smokers of unfiltered cigarettes (RR = 0.36, CI = 0.18-0.75)."
Falk et al., in a study of the risk for laryngeal cancer, found that: "Higher risks were associated with smoking nonfiltered than filtered cigarettes." For those who smoked filtered cigarettes, the OR was 5.9 (95% CI = 2.4-14.4); for those who smoked non-filtered cigarettes, the OR was 9.0 (95% CI = 3.2-25.1).
Luchtenborg et al. found that while non-filtered cigarettes increased the risk for colon cancer (OR 1.59; 95% CI, 1.15-2.21; P(trend) = 0.001), filtered cigarettes did not increase colon cancer risk (OR 1.05; 95% CI, 0.79-1.39; P(trend) = 0.98).
Wynder et al. reported slightly lower bladder cancer risk among filtered cigarette smokers: "Smokers of filtered cigarettes had a slightly reduced risk of bladder cancer relative to smokers of nonfiltered cigarettes (odds ratio 0.64, 95% confidence interval 0.38 to 1.10 among male smokers; odds ratio 0.74, 95% confidence interval 0.37 to 1.48 among female smokers)."
Hartge et al. found exactly the same result as Wynder's group: "Our data indicated that people who have only smoked unfiltered cigarettes have higher risks."
Sadly, although the Surgeon General's report draws conclusions about the health impact of filtered cigarettes, it only cites one of these seven studies (the Luchtenborg study). And in citing that study, the report merely notes its finding that smoking increases colon cancer risk. It hides this study's finding that this increased colon cancer risk was only detected among smokers of non-filtered cigarettes!
Why does the Surgeon General's report not review the literature on the cancer risks of filtered vs. non-filtered cigarettes, even though it seems to draw a conclusion about this issue? The only answer I can think of is that the report aimed to draw a particular conclusion, rather than to present the facts in an objective way. Apparently, the report was pre-determined to conclude that all design changes to cigarettes increased their cancer risk. It conflated the filter with other sources of tar yield reductions and at the same time, failed to review studies that examined the relative risk of filtered vs. non-filtered cigarettes.
As a result, the report implies that cigarette filters increase lung cancer risk and opens the way for lawsuits based on this claim, as the Law360.com article suggests.
But the truth is more nuanced. While there is no question that low-tar or "light" cigarettes are not safer, it is not the case that the introduction of filters made cigarettes more carcinogenic. I would not be able to testify in a courtroom that I believe filtered cigarettes are more dangerous than non-filtered cigarettes. Nor would I be able to testify that filtered cigarettes and non-filtered cigarettes pose equivalent cancer risk.
It is important to point out that just because the relative risk of cancer associated with filtered cigarettes is lower than that for non-filtered cigarettes, it does not necessarily follow that switching from a non-filtered to a filtered cigarette will reduce one's health risks. It is possible that smokers who make such a switch will compensate because they are used to higher tar levels. It is possible that the observed reduction in cancer risk only holds for lifelong filtered cigarette smokers, as they do not compensate (they never smoked non-filtered cigarettes). In fact, the scientific evidence supports this contention.
The rest of the story is that in yet another area of tobacco control science, the Surgeon General's report is providing a biased view of the scientific evidence.
Thursday, January 23, 2014
CDC is Intentionally Hiding Conflicts of Interest of Surgeon General's Report Authors
Earlier this week, I revealed that the 2014 Surgeon General's report fails to disclose the conflicts of interest of its authors, many of whom have received money from pharmaceutical companies which manufacture the very products about which the report opines. I also explained how this is particularly problematic, since the report itself complains about how historically, tobacco-funded scientists failed
to disclose their conflicts of interest. I concluded that the 2014 Surgeon General's report is violating the very ethical
principles that it attacks the tobacco company for violating in the
past, and I note that while there has been substantial progress in the past 50 years in
the area of disclosure of conflicts of interest, somehow that progress
has evaded the producers of the Surgeon General's report itself.
Today, I reveal that the CDC's Office on Smoking and Health (OSH) - the lead agency that produces the report - is apparently intentionally hiding the conflicts of interest. In other words, OSH knows about these conflicts but has apparently decided not to share this information with the public. That is, OSH is intentionally hiding these conflicts from the public.
The Rest of the Story
Yesterday, I was informed by one of the contributing authors to the 2014 Surgeon General's report that each of the authors and reviewers of the report was required to complete conflict of interest disclosure forms. This makes the problem even more serious than it initially appeared. It now seems that this is not merely a matter of the CDC not knowing about, or failing to inquire about the conflicts of interest of report authors. Instead, this is now a matter of the CDC hiding, or covering up, these conflicts of interest, which are not revealed to the public anywhere in the report or on the report's web site.
There is no excuse for collecting this important information, but not revealing it to the public. The only legitimate justification for this would be if there were no reported conflicts of interest. In such a case, the report could have included a statement indicating that none of the report's authors reported a conflict of interest.
But we know this is not the case because in journal articles published by many of the report authors, they have acknowledged multiple conflicts of interest with Big Pharma.
Let's just take three of the Surgeon General's report authors alone (Dr. Neal Benowitz, Dr. Jack Henningfield, and Dr. Jonathan Samet). According to a D.C. District Court brief filed by R.J. Reynolds and Lorillard:
Dr. Benowitz: "Dr. Benowitz, as a paid consultant for pharmaceutical companies, has assisted them with the design, development, and marketing of smoking-cessation products. Among the companies for which he has consulted on such products are GlaxoSmithKline plc and its affiliates (collectively, “GSK”); Pfizer, Inc. and its affiliates (collectively, “Pfizer”); Novartis AG and its affiliates (collectively, “Novartis”); Sanofi-Aventis U.S. LLC and its affiliates (collectively, “Sanofi-Aventis”); and Aradigm Corp. and its affiliates (collectively, “Aradigm”). During the last ten years, he has received at least approximately $10,000 per year for such consulting. He has also received grant support for research and writing from GSK and/or Pfizer on at least five occasions. In 2010, he co-authored a study, funded by Pfizer, on the use of its drug, Chantix, for smoking cessation."
Dr. Henningfield: "Dr. Henningfield is a Principal at, and derives most of his income from, Pinney Associates, a firm that currently provides to GSK on an exclusive basis consulting services regarding smoking-cessation products. His formal title is: Vice President, Research & Health Policy. Through his association with Pinney Associates, Dr. Henningfield advises GSK specifically on the development of nicotine-replacement therapies and treatments for tobacco dependence. Pinney Associates has received on average more than $2 million per year in revenue from pharmaceutical companies, more than half of which relates to smoking-cessation products. In addition, during the last decade, Dr. Henningfield has received grant support for research and writing from GSK on at least eight occasions. Dr. Henningfield is also a partner in a company that holds patents for a nicotine replacement-therapy product. He has estimated that, if thess patents are successfully licensed, they could be worth more than $1 million to him as a partner in that company. Thus, Dr. Henningfield has a financial interest in bringing about regulatory policies that will drive current smokers to use nicotine-replacement-therapy products."
Dr. Samet: "During the last decade, Dr. Samet has received grant support for research and writing from GSK on at least six occasions, including in 2010. In addition, he formerly led the Institute for Global Tobacco Control, which is funded by GSK and Pfizer. Moreover, until 2009, Dr. Samet received regular honoraria from Pfizer for his service on the Pfizer Global Tobacco Advisory Board."
Thus, as revealed and described in this lawsuit brief and in an accompanying press release: "Drs. Neil Benowitz, Jack E. Henningfield and Jonathan M. Samet are conflicted ... due to their continuing financial relationships with pharmaceutical companies that make smoking-cessation products."
Incidentally, the Reynolds/Lorillard lawsuit seeks to have Drs. Benowitz, Henningfield, and Samet dismissed from the FDA's TPSAC (Tobacco Product Scientific Advisory Committee) panel because of these conflicts of interest. While these conflicts do not preclude the participation of these scientists as authors of the Surgeon General's report, they absolutely must be disclosed to the public.
To make matters worse, Dr. Samet is not just an author, but served as one of the two editors of the report.
The rest of the story is that not only is CDC failing to disclose the important conflicts of interest of the 2014 Surgeon General's report authors, but OSH is involved in a cover-up. Apparently, OSH has deliberately chosen to hide these conflicts of interest from the public.
It may take a Freedom of Interest Act (FOIA) request to obtain this information from OSH, or wherever this "secret" information resides, which is quite a shame given the fact that one of the major points made in the Surgeon General's report is its criticism of the unethical behavior of tobacco industry scientists who hid their financial relationships with the industry. It's sad that the federal government is condemning the past actions of scientists who hid financial connections with Big Tobacco, while it is engaging in the present action of hiding financial connections with Big Pharma.
Today, I reveal that the CDC's Office on Smoking and Health (OSH) - the lead agency that produces the report - is apparently intentionally hiding the conflicts of interest. In other words, OSH knows about these conflicts but has apparently decided not to share this information with the public. That is, OSH is intentionally hiding these conflicts from the public.
The Rest of the Story
Yesterday, I was informed by one of the contributing authors to the 2014 Surgeon General's report that each of the authors and reviewers of the report was required to complete conflict of interest disclosure forms. This makes the problem even more serious than it initially appeared. It now seems that this is not merely a matter of the CDC not knowing about, or failing to inquire about the conflicts of interest of report authors. Instead, this is now a matter of the CDC hiding, or covering up, these conflicts of interest, which are not revealed to the public anywhere in the report or on the report's web site.
There is no excuse for collecting this important information, but not revealing it to the public. The only legitimate justification for this would be if there were no reported conflicts of interest. In such a case, the report could have included a statement indicating that none of the report's authors reported a conflict of interest.
But we know this is not the case because in journal articles published by many of the report authors, they have acknowledged multiple conflicts of interest with Big Pharma.
Let's just take three of the Surgeon General's report authors alone (Dr. Neal Benowitz, Dr. Jack Henningfield, and Dr. Jonathan Samet). According to a D.C. District Court brief filed by R.J. Reynolds and Lorillard:
Dr. Benowitz: "Dr. Benowitz, as a paid consultant for pharmaceutical companies, has assisted them with the design, development, and marketing of smoking-cessation products. Among the companies for which he has consulted on such products are GlaxoSmithKline plc and its affiliates (collectively, “GSK”); Pfizer, Inc. and its affiliates (collectively, “Pfizer”); Novartis AG and its affiliates (collectively, “Novartis”); Sanofi-Aventis U.S. LLC and its affiliates (collectively, “Sanofi-Aventis”); and Aradigm Corp. and its affiliates (collectively, “Aradigm”). During the last ten years, he has received at least approximately $10,000 per year for such consulting. He has also received grant support for research and writing from GSK and/or Pfizer on at least five occasions. In 2010, he co-authored a study, funded by Pfizer, on the use of its drug, Chantix, for smoking cessation."
Dr. Henningfield: "Dr. Henningfield is a Principal at, and derives most of his income from, Pinney Associates, a firm that currently provides to GSK on an exclusive basis consulting services regarding smoking-cessation products. His formal title is: Vice President, Research & Health Policy. Through his association with Pinney Associates, Dr. Henningfield advises GSK specifically on the development of nicotine-replacement therapies and treatments for tobacco dependence. Pinney Associates has received on average more than $2 million per year in revenue from pharmaceutical companies, more than half of which relates to smoking-cessation products. In addition, during the last decade, Dr. Henningfield has received grant support for research and writing from GSK on at least eight occasions. Dr. Henningfield is also a partner in a company that holds patents for a nicotine replacement-therapy product. He has estimated that, if thess patents are successfully licensed, they could be worth more than $1 million to him as a partner in that company. Thus, Dr. Henningfield has a financial interest in bringing about regulatory policies that will drive current smokers to use nicotine-replacement-therapy products."
Dr. Samet: "During the last decade, Dr. Samet has received grant support for research and writing from GSK on at least six occasions, including in 2010. In addition, he formerly led the Institute for Global Tobacco Control, which is funded by GSK and Pfizer. Moreover, until 2009, Dr. Samet received regular honoraria from Pfizer for his service on the Pfizer Global Tobacco Advisory Board."
Thus, as revealed and described in this lawsuit brief and in an accompanying press release: "Drs. Neil Benowitz, Jack E. Henningfield and Jonathan M. Samet are conflicted ... due to their continuing financial relationships with pharmaceutical companies that make smoking-cessation products."
Incidentally, the Reynolds/Lorillard lawsuit seeks to have Drs. Benowitz, Henningfield, and Samet dismissed from the FDA's TPSAC (Tobacco Product Scientific Advisory Committee) panel because of these conflicts of interest. While these conflicts do not preclude the participation of these scientists as authors of the Surgeon General's report, they absolutely must be disclosed to the public.
To make matters worse, Dr. Samet is not just an author, but served as one of the two editors of the report.
The rest of the story is that not only is CDC failing to disclose the important conflicts of interest of the 2014 Surgeon General's report authors, but OSH is involved in a cover-up. Apparently, OSH has deliberately chosen to hide these conflicts of interest from the public.
It may take a Freedom of Interest Act (FOIA) request to obtain this information from OSH, or wherever this "secret" information resides, which is quite a shame given the fact that one of the major points made in the Surgeon General's report is its criticism of the unethical behavior of tobacco industry scientists who hid their financial relationships with the industry. It's sad that the federal government is condemning the past actions of scientists who hid financial connections with Big Tobacco, while it is engaging in the present action of hiding financial connections with Big Pharma.
Wednesday, January 22, 2014
Why Did Surgeon General's Report Violate Well-Accepted Ethical Guidelines for Disclosing Conflicts of Interest?
Yesterday, I revealed that the 2014 Surgeon General's report, released last Friday, failed to disclose the financial conflicts of interest of many of its authors. Specifically, the report is hiding the fact that many of its authors have or had
financial conflicts of interest with pharmaceutical companies that
manufacture the smoking cessation products about which the report provides a misleadingly
positive review.
The Rest of the Story
The failure of the report to disclose financial conflicts of interests of its authors is problematic for several reasons.
First, disclosure of conflicts of interest has become a widely accepted guideline for ethical practice in medicine and public health. Most, if not all, reputable public health and medical journals require authors to disclose any relevant conflicts of interest and most journals publish any conflicts that are disclosed.
Second, disclosure of conflicts of interest is essential to achieve the public health ethical principle of transparency. Readers have the right to know if there are any relevant conflicts that could be perceived as influencing the objectivity of scientific reports.
Third, the Surgeon General's report comes across as a project of massive hypocrisy, as the report itself complains about how tobacco-funded scientists failed to disclose their conflicts of interest. The report emphasizes that in the 50 years since the release of the report, disclosure of financial conflicts has become the "norm." It bemoans the fact that in the past, tobacco-funded scientists did not disclose their conflicts of interest, which left readers unaware of these important financial relationships.
According to the Surgeon General's report:
"Engagement with the industry became increasingly unacceptable for researchers whose reputations were tarnished by their industry activities. At the same time, concerns about potential conflicts of interest among scientists increased, and disclosure of consulting activities to universities became the norm, making it more difficult for researchers to maintain secret ties to the tobacco industry. By contrast, when the 1964 report was released, there was little concern that scientists’ results would be influenced by their funding source." ...
While disclosure of consulting activities may have become the norm, it certainly has not become the norm for the Surgeon General's report!
The report goes on to state:
"It is difficult to estimate the extent to which industry-generated research activities have influenced scientific thinking regarding the effects of nicotine on cognitive performance and on nicotine’s therapeutic applications. Authors’ industry affiliations and potential conflicts of interest reported in publications may go unnoticed by readers, may be difficult to identify, or may not be disclosed at all. Reviews and other articles citing industry-affiliated studies generally did not include author affiliations or potential conflicts of interest at all, leaving the readers unaware of possible industry influences."
Unfortunately, the 2014 Surgeon General's report has left readers unaware of possible industry influences, as it has failed to disclose the pharmaceutical industry ties of many of its authors. And it is not difficult to estimate the extent to which pharmaceutical industry-generated research activities have influenced scientific thinking regarding the effects of smoking cessation drugs and nicotine's therapeutic (cessation) applications.
The rest of the story is that the 2014 Surgeon General's report is violating the very ethical principles that it attacks the tobacco company for violating in the past. While there has been substantial progress in the past 50 years in the area of disclosure of conflicts of interest, somehow that progress has evaded the producers of the Surgeon General's report itself.
The Rest of the Story
The failure of the report to disclose financial conflicts of interests of its authors is problematic for several reasons.
First, disclosure of conflicts of interest has become a widely accepted guideline for ethical practice in medicine and public health. Most, if not all, reputable public health and medical journals require authors to disclose any relevant conflicts of interest and most journals publish any conflicts that are disclosed.
Second, disclosure of conflicts of interest is essential to achieve the public health ethical principle of transparency. Readers have the right to know if there are any relevant conflicts that could be perceived as influencing the objectivity of scientific reports.
Third, the Surgeon General's report comes across as a project of massive hypocrisy, as the report itself complains about how tobacco-funded scientists failed to disclose their conflicts of interest. The report emphasizes that in the 50 years since the release of the report, disclosure of financial conflicts has become the "norm." It bemoans the fact that in the past, tobacco-funded scientists did not disclose their conflicts of interest, which left readers unaware of these important financial relationships.
According to the Surgeon General's report:
"Engagement with the industry became increasingly unacceptable for researchers whose reputations were tarnished by their industry activities. At the same time, concerns about potential conflicts of interest among scientists increased, and disclosure of consulting activities to universities became the norm, making it more difficult for researchers to maintain secret ties to the tobacco industry. By contrast, when the 1964 report was released, there was little concern that scientists’ results would be influenced by their funding source." ...
While disclosure of consulting activities may have become the norm, it certainly has not become the norm for the Surgeon General's report!
The report goes on to state:
"It is difficult to estimate the extent to which industry-generated research activities have influenced scientific thinking regarding the effects of nicotine on cognitive performance and on nicotine’s therapeutic applications. Authors’ industry affiliations and potential conflicts of interest reported in publications may go unnoticed by readers, may be difficult to identify, or may not be disclosed at all. Reviews and other articles citing industry-affiliated studies generally did not include author affiliations or potential conflicts of interest at all, leaving the readers unaware of possible industry influences."
Unfortunately, the 2014 Surgeon General's report has left readers unaware of possible industry influences, as it has failed to disclose the pharmaceutical industry ties of many of its authors. And it is not difficult to estimate the extent to which pharmaceutical industry-generated research activities have influenced scientific thinking regarding the effects of smoking cessation drugs and nicotine's therapeutic (cessation) applications.
The rest of the story is that the 2014 Surgeon General's report is violating the very ethical principles that it attacks the tobacco company for violating in the past. While there has been substantial progress in the past 50 years in the area of disclosure of conflicts of interest, somehow that progress has evaded the producers of the Surgeon General's report itself.
Tuesday, January 21, 2014
New Surgeon General's Report Hides Studies on Unaided Smoking Cessation and Hides Conflicts of Interest of Report Authors
Despite its massive 978-page length, the new Surgeon General's report - released last Friday - fails to include any mention of the many population-based studies which have shown that unaided smoking cessation is superior to the use of nicotine replacement therapy (NRT).
This glaring omission in the report was first revealed in a detailed and insightful commentary by John Polito, at whyquit.com.
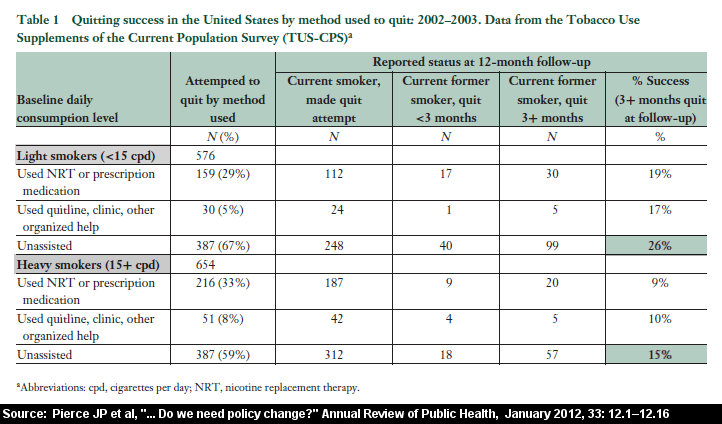
Polito writes: "Physicians and government health workers are asked to ignore the fact that, as found by a July 2013 Gallup Poll, more patients quit smoking cold turkey than by all other methods combined, that only a tiny fraction of successful cessation involves use of any approved product (just 8 percent). Reflect on the fact that after 30 years and billions spent marketing Nicorette, that the Gallup Poll found that only 1 in 100 succeeded via nicotine gum. ... Fifty years of progress? Survey after survey teaches that feeding nicotine to nicotine addicts has nailed cessation to the floor, and that force-feeding weaning programs are costing lives (see Doran 2006, Hartman 2006, West 2006, Cheong 2007, Ferguson 2009, Pierce 2012). Don't expect to find any abrupt nicotine cessation paper cited in the General's 978 page report. None. Why? Because the 50th Anniversary Surgeon General report invited a number of financially conflicted researchers to help write it. Although impossible to know the role each played, to these eyes, their master's bidding leaps from the report."
Polito includes a table which compares the cessation success rates of unaided quitting compared to drugs in population-based studies. For heavy smokers, NRT achieves a 9% success rate compared to 15% for unassisted quitting.
This information is not included in the massive report.
The Rest of the Story
The inferiority of drugs to abrupt cold turkey quitting is not the only thing that the massive Surgeon General's report is hiding.
The report is also hiding the fact that many of its authors have or had financial conflicts of interest with pharmaceutical companies that manufacture the products about which the report provides a misleadingly positive review.
In fact, the report fails to disclose any of the many conflicts of interest of its authors with Big Pharma.
This lack of transparency in the report is unfortunate because readers deserve to be informed about financial conflicts of interest that could potentially have influenced the report's presentation and interpretation of the scientific evidence. This is especially important because the report makes broad conclusions regarding national strategies for smoking cessation. Thus, if the report's authors have received money from pharmaceutical companies that make the very products about which the report is opining, it would be critical to disclose these conflicts. The report fails to do so.
This not only supports Polito's hypothesis that the report's blatant bias in reporting on smoking cessation is due to the financial conflicts of its authors, who were doing their "master's bidding," but it also suggests that the producers of this report truly have something to hide.
This glaring omission in the report was first revealed in a detailed and insightful commentary by John Polito, at whyquit.com.
Polito writes: "Physicians and government health workers are asked to ignore the fact that, as found by a July 2013 Gallup Poll, more patients quit smoking cold turkey than by all other methods combined, that only a tiny fraction of successful cessation involves use of any approved product (just 8 percent). Reflect on the fact that after 30 years and billions spent marketing Nicorette, that the Gallup Poll found that only 1 in 100 succeeded via nicotine gum. ... Fifty years of progress? Survey after survey teaches that feeding nicotine to nicotine addicts has nailed cessation to the floor, and that force-feeding weaning programs are costing lives (see Doran 2006, Hartman 2006, West 2006, Cheong 2007, Ferguson 2009, Pierce 2012). Don't expect to find any abrupt nicotine cessation paper cited in the General's 978 page report. None. Why? Because the 50th Anniversary Surgeon General report invited a number of financially conflicted researchers to help write it. Although impossible to know the role each played, to these eyes, their master's bidding leaps from the report."
{kind=link}
Polito includes a table which compares the cessation success rates of unaided quitting compared to drugs in population-based studies. For heavy smokers, NRT achieves a 9% success rate compared to 15% for unassisted quitting.
This information is not included in the massive report.
The Rest of the Story
The inferiority of drugs to abrupt cold turkey quitting is not the only thing that the massive Surgeon General's report is hiding.
The report is also hiding the fact that many of its authors have or had financial conflicts of interest with pharmaceutical companies that manufacture the products about which the report provides a misleadingly positive review.
In fact, the report fails to disclose any of the many conflicts of interest of its authors with Big Pharma.
This lack of transparency in the report is unfortunate because readers deserve to be informed about financial conflicts of interest that could potentially have influenced the report's presentation and interpretation of the scientific evidence. This is especially important because the report makes broad conclusions regarding national strategies for smoking cessation. Thus, if the report's authors have received money from pharmaceutical companies that make the very products about which the report is opining, it would be critical to disclose these conflicts. The report fails to do so.
This not only supports Polito's hypothesis that the report's blatant bias in reporting on smoking cessation is due to the financial conflicts of its authors, who were doing their "master's bidding," but it also suggests that the producers of this report truly have something to hide.
Monday, January 20, 2014
FDA to Protect Americans from "Defective" Cigarettes, But Not from "Normal" Deadly Cigarettes
In a move that sounds more like a headline in the Onion than an act of a federal health protection agency, the FDA has announced that it is going to protect the public from the dangers of "defective" cigarettes.
What is a defective cigarette, you may ask. Well, according to the FDA, a cigarette that causes lung cancer, heart disease, emphysema, kidney cancer, or leukemia is not defective. Those are cigarettes which are working the way they are supposed to work!
A defective cigarette is one which causes health effects "beyond those normally associated with tobacco product use."
Further, the FDA is asking smokers who suffer such extra-ordinary health effects to report them to the agency. But the FDA doesn't want to hear from you if you simply suffer a "normal" health effect, like crippling obstructive lung disease, inability to breathe, metastatic cancer, or brain infarctions. In order to engage the FDA's interest, the health problem must be one that is beyond these "normal" product side effects.
What would be an example of such a severe problem that it warrants reporting to the FDA? According to the medical branch chief in the Office of Science at FDA's Center for Tobacco Products, such a severe problem would be something like if a cigarette "just smells or tastes wrong."
The Rest of the Story
What a great public health accomplishment it was to put cigarettes under the jurisdiction of the Food and Drug Administration. Although the FDA has so far done not a single thing to address cigarette safety problems such as heart disease, lung disease, and cancer, we can all breathe easier knowing that the FDA will plunge into action if a smoker somewhere reports that a cigarette doesn't smell or taste right.
While the FDA has given its official stamp of approval to the "normal" cigarettes that are killing more than 400,000 Americans each year and has taken no action to reduce the hazards of smoking, we can all be grateful that the agency has stepped in to protect the public from cigarettes that smell or taste wrong.
The FDA's Center for Tobacco Products (CTP) assures us that for defective cigarettes, such as those which taste wrong, "issues will be addressed to ensure the protection of the public health." However, for normal cigarettes that are merely toxic or deadly, the FDA has taken no action to date to require these products to be safer.
Frankly, as I predicted prior to the enactment of the Family Smoking Prevention and Tobacco Control Act, the FDA's regulation of tobacco products is a national public health embarrassment.
Perhaps the FDA Center for Tobacco Products' slogan should be: "CTP: Protecting the Public from Cigarettes that Smell Wrong."
What is a defective cigarette, you may ask. Well, according to the FDA, a cigarette that causes lung cancer, heart disease, emphysema, kidney cancer, or leukemia is not defective. Those are cigarettes which are working the way they are supposed to work!
A defective cigarette is one which causes health effects "beyond those normally associated with tobacco product use."
Further, the FDA is asking smokers who suffer such extra-ordinary health effects to report them to the agency. But the FDA doesn't want to hear from you if you simply suffer a "normal" health effect, like crippling obstructive lung disease, inability to breathe, metastatic cancer, or brain infarctions. In order to engage the FDA's interest, the health problem must be one that is beyond these "normal" product side effects.
What would be an example of such a severe problem that it warrants reporting to the FDA? According to the medical branch chief in the Office of Science at FDA's Center for Tobacco Products, such a severe problem would be something like if a cigarette "just smells or tastes wrong."
The Rest of the Story
What a great public health accomplishment it was to put cigarettes under the jurisdiction of the Food and Drug Administration. Although the FDA has so far done not a single thing to address cigarette safety problems such as heart disease, lung disease, and cancer, we can all breathe easier knowing that the FDA will plunge into action if a smoker somewhere reports that a cigarette doesn't smell or taste right.
While the FDA has given its official stamp of approval to the "normal" cigarettes that are killing more than 400,000 Americans each year and has taken no action to reduce the hazards of smoking, we can all be grateful that the agency has stepped in to protect the public from cigarettes that smell or taste wrong.
The FDA's Center for Tobacco Products (CTP) assures us that for defective cigarettes, such as those which taste wrong, "issues will be addressed to ensure the protection of the public health." However, for normal cigarettes that are merely toxic or deadly, the FDA has taken no action to date to require these products to be safer.
Frankly, as I predicted prior to the enactment of the Family Smoking Prevention and Tobacco Control Act, the FDA's regulation of tobacco products is a national public health embarrassment.
Perhaps the FDA Center for Tobacco Products' slogan should be: "CTP: Protecting the Public from Cigarettes that Smell Wrong."
Thursday, January 16, 2014
Anti-Smoking Advocate/Professor Calls for Ban on Electronic Cigarette Advertising, But Not Advertising for Deadly Tobacco Cigarettes
In an op-ed piece published in the Milwaukee Journal-Sentinel, professor of epidemiology Dr. Ruth Etzel - formerly with the World Health Organization - called for a ban on electronic cigarette advertising. However, she made no similar call for a ban on tobacco cigarette advertising.
In the piece, she writes: "E-cigarettes are marketed in a variety of flavors, including cherry crush, peach schnapps, java jolt and magnificent menthol; such flavoring agents increase the appeal of the product to youth. Not surprisingly, the use of e-cigarettes is rapidly increasing among children. This is why this "next generation" product is of concern to pediatricians like myself; it offers an excellent way to addict the next generation of children to nicotine. ... We are at a critical juncture now — a moment when we can prevent children from being duped by advertising into using e-cigarettes. We should take steps to ban the advertising of e-cigarettes and prohibit their use indoors to ensure that the next generation does not suffer the consequences."
The Rest of the Story
While Dr. Etzel seems to be quite concerned about youth use of e-cigarettes, she fails to display a similar level of concern about youth using tobacco cigarettes. In fact, while she calls for a ban on electronic cigarette advertising to protect youths from possible nicotine addiction, she makes no similar call for a ban on tobacco advertising, which we know leads many youths to definite nicotine addiction.
What possible justification is there for banning advertising for electronic cigarettes, but not for the real thing?
This story illustrates how misguided anti-smoking efforts are at the present time. We are placing a huge emphasis on trying to protect kids from e-cigarettes, but losing our focus on preventing kids from becoming addicted to smoking, a behavior that will eventually kill half of those who become regular users.
While anti-smoking groups push for bans on vaping in all workplaces and public places - even outdoor parks - throughout the nation, they are doing virtually nothing about the problem of secondhand smoke that is actually killing people: nearly half of the states still fail to protect workers from tobacco smoke exposure in bars, restaurants, and/or casinos.
It is also important to mention that banning electronic cigarette advertising would violate the First Amendment rights of e-cigarette companies.
Instead, what we need are FDA regulations that will prevent the marketing of electronic cigarettes to youth. An outright ban on e-cigarette advertising is neither sensible nor constitutional.
More importantly, we need anti-smoking groups to once again become anti-smoking. Electronic cigarettes are devices which are helping thousands of smokers to get off cigarettes. Groups which oppose these products are opposing a viable form of smoking cessation. This is tantamount to being pro-smoking.
Instead of worrying about banning electronic cigarettes in every park, sidewalk, and beach in the country, anti-smoking groups should get back to the business of trying to reduce smoking: that means focusing on promoting smoke-free workplaces in the states that still don't offer such protection and embracing e-cigarettes as a smoking cessation and harm reduction strategy.
To be sure, the FDA should prohibit the marketing of electronic cigarettes to youth. But a total ban on electronic cigarette advertising would be throwing away the baby with the bath water.
Why so many tobacco control advocates want to protect cigarettes from competition is baffling to me.
In the piece, she writes: "E-cigarettes are marketed in a variety of flavors, including cherry crush, peach schnapps, java jolt and magnificent menthol; such flavoring agents increase the appeal of the product to youth. Not surprisingly, the use of e-cigarettes is rapidly increasing among children. This is why this "next generation" product is of concern to pediatricians like myself; it offers an excellent way to addict the next generation of children to nicotine. ... We are at a critical juncture now — a moment when we can prevent children from being duped by advertising into using e-cigarettes. We should take steps to ban the advertising of e-cigarettes and prohibit their use indoors to ensure that the next generation does not suffer the consequences."
The Rest of the Story
While Dr. Etzel seems to be quite concerned about youth use of e-cigarettes, she fails to display a similar level of concern about youth using tobacco cigarettes. In fact, while she calls for a ban on electronic cigarette advertising to protect youths from possible nicotine addiction, she makes no similar call for a ban on tobacco advertising, which we know leads many youths to definite nicotine addiction.
What possible justification is there for banning advertising for electronic cigarettes, but not for the real thing?
This story illustrates how misguided anti-smoking efforts are at the present time. We are placing a huge emphasis on trying to protect kids from e-cigarettes, but losing our focus on preventing kids from becoming addicted to smoking, a behavior that will eventually kill half of those who become regular users.
While anti-smoking groups push for bans on vaping in all workplaces and public places - even outdoor parks - throughout the nation, they are doing virtually nothing about the problem of secondhand smoke that is actually killing people: nearly half of the states still fail to protect workers from tobacco smoke exposure in bars, restaurants, and/or casinos.
It is also important to mention that banning electronic cigarette advertising would violate the First Amendment rights of e-cigarette companies.
Instead, what we need are FDA regulations that will prevent the marketing of electronic cigarettes to youth. An outright ban on e-cigarette advertising is neither sensible nor constitutional.
More importantly, we need anti-smoking groups to once again become anti-smoking. Electronic cigarettes are devices which are helping thousands of smokers to get off cigarettes. Groups which oppose these products are opposing a viable form of smoking cessation. This is tantamount to being pro-smoking.
Instead of worrying about banning electronic cigarettes in every park, sidewalk, and beach in the country, anti-smoking groups should get back to the business of trying to reduce smoking: that means focusing on promoting smoke-free workplaces in the states that still don't offer such protection and embracing e-cigarettes as a smoking cessation and harm reduction strategy.
To be sure, the FDA should prohibit the marketing of electronic cigarettes to youth. But a total ban on electronic cigarette advertising would be throwing away the baby with the bath water.
Why so many tobacco control advocates want to protect cigarettes from competition is baffling to me.
Wednesday, January 15, 2014
Rest of the Story Reaches Consensus on Corrective Statements for CDC and Anti-Smoking Groups
According to an article at CSPnet.com: "The nation's tobacco companies and the U.S. Department of Justice (DOJ)
have reached an agreement on publishing corrective statements that say
the companies lied about the dangers of smoking and requires them to
disclose smoking's health effects, said an Associated Press report."
The article reports that: "Under the agreement with the DOJ, each of the companies must publish full-page ads in the Sunday editions of 35 newspapers and on the newspapers' websites, as well as air prime-time TV spots on CBS, ABC or NBC five times per week for a year. The companies also must publish the statements on their websites and affix them to a certain number of cigarette packs three times per year for two years."
"Each corrective ad is to be prefaced by a statement that a federal court has concluded that the defendant tobacco companies 'deliberately deceived the American public.' Among the required statements are that smoking kills more people than murder, AIDS, suicide, drugs, car crashes and alcohol combined, and that 'secondhand smoke kills over 38,000 Americans a year.'"
The Rest of the Story
At the same time that the tobacco companies and the U.S. Department of Justice reached a consensus on the location of the tobacco industry corrective statements, the Rest of the Story has reached a consensus on the text and location of a set of corrective statements it is ordering that CDC and several anti-smoking groups and advocates make, in the wake of last year's revelation that they lied about the dangers of electronic cigarettes.
The consensus, which was reached over the weekend, requires public corrective statements from the CDC, the Mayo Clinic, Dr. Stan Glantz, and the University of Kentucky Cancer Center.
The required text for the corrective statements and their required placement is as follows:
For CDC:
The Rest of the Story has ruled that the Centers for Disease Control and Prevention has lied to the American public by telling them that studies have demonstrated electronic cigarettes are a gateway to a lifetime addiction to smoking, and has ordered the CDC to make this statement. Here is the truth:
• We lied to you when we told you that "many kids are starting out with e-cigarettes and then going on to smoke conventional cigarettes."
• The truth is that the study we relied upon did not measure the time course of electronic cigarette and cigarette use. Thus, it could not determine whether the kids who were using both cigarettes and electronic cigarettes had initiated with smoking or with electronic cigarettes.
• The only study to examine this question found that e-cigarettes are not a gateway to smoking.
• There is no evidence at the current time that kids are starting out with e-cigarettes and then going on to smoke conventional cigarettes.
Placement:
1. Medscape - where the original interview with Dr. Frieden appears
2. The 52 media outlets that carried the story and quoted Dr. Frieden as stating that electronic cigarettes are "condemning many kids to struggling with a lifelong addiction to nicotine."
3. CDC web site
For the Mayo Clinic:
The Rest of the Story has ruled that the Mayo Clinic has lied to the American public by telling them that absolutely no studies have examined the health effects of electronic cigarettes and that doctors have no way of assessing the impact of this product, and has ordered the Mayo Clinic to make this statement. Here is the truth:
• We lied to you when we told you that "No studies have been done to examine the safety of e-cigarettes."
• The truth is that there are at least 10 published studies that examined the health effects of electronic cigarettes. And this doesn't even include the more than 20 studies in which the chemical constituents of electronic cigarette liquids or vapor have been analyzed using gas chromatography/mass spectrometry.
• We also lied to you when we told you that "with nicotine inhalers you receive only nicotine."
• The truth is that nicotine inhalers deliver to users the following chemicals:
Formaldehyde
Acetaldehyde
o-methylbenzene
Cadmium
Nickel
Lead
Placement:
1. Mayo Clinic web site
2. Mayo Clinic Proceedings
For Stan Glantz:
The Rest of the Story has ruled that I lied to the American public by telling them that studies have demonstrated electronic cigarette experimentation leads to nicotine addiction among nonsmokers who try these products, and has ordered me to make this statement. Here is the truth:
• I lied to you when I told you that in the Choi and Forster study, "e-cigarettes were a pathway to renewed or new nicotine addiction."
• The truth is that the study only measured ever use of electronic cigarettes, not current use, regular use, or addiction to nicotine. Thus, it could not determine whether the kids who had tried electronic cigarettes ever used them again. So it could not tell if these kids were addicted to nicotine. They may have simply tried an electronic cigarette and not vaped again.
• I also lied to you when I told you that my own study demonstrated that electronic cigarettes are "a new route to smoking addiction for adolescents." The study was a cross-sectional one, so I could not draw that conclusion. And I admitted it in the article itself. But that's not what I told you.
Placement:
1. Stan Glantz blog
2. Stan Glantz announcement list
3. UCSF web site
For the University of Kentucky Cancer Center:
The Rest of the Story has ruled that we lied to the American public by telling them that electronic cigarettes are every bit as harmful as smoking, and has ordered us to make this statement. Here is the truth:
• We lied to you when we told you that electronic cigarettes may be "every bit as dangerous" as tobacco cigarettes.
• The truth is that there is abundant evidence that electronic cigarettes are much safer than regular cigarettes. Even the tobacco industry itself acknowledges that smoking is more hazardous than vaping.
Placement:
1. University of Kentucky Cancer Center web site
2. Letter to all Kentucky state legislators
The article reports that: "Under the agreement with the DOJ, each of the companies must publish full-page ads in the Sunday editions of 35 newspapers and on the newspapers' websites, as well as air prime-time TV spots on CBS, ABC or NBC five times per week for a year. The companies also must publish the statements on their websites and affix them to a certain number of cigarette packs three times per year for two years."
"Each corrective ad is to be prefaced by a statement that a federal court has concluded that the defendant tobacco companies 'deliberately deceived the American public.' Among the required statements are that smoking kills more people than murder, AIDS, suicide, drugs, car crashes and alcohol combined, and that 'secondhand smoke kills over 38,000 Americans a year.'"
The Rest of the Story
At the same time that the tobacco companies and the U.S. Department of Justice reached a consensus on the location of the tobacco industry corrective statements, the Rest of the Story has reached a consensus on the text and location of a set of corrective statements it is ordering that CDC and several anti-smoking groups and advocates make, in the wake of last year's revelation that they lied about the dangers of electronic cigarettes.
The consensus, which was reached over the weekend, requires public corrective statements from the CDC, the Mayo Clinic, Dr. Stan Glantz, and the University of Kentucky Cancer Center.
The required text for the corrective statements and their required placement is as follows:
For CDC:
The Rest of the Story has ruled that the Centers for Disease Control and Prevention has lied to the American public by telling them that studies have demonstrated electronic cigarettes are a gateway to a lifetime addiction to smoking, and has ordered the CDC to make this statement. Here is the truth:
• We lied to you when we told you that "many kids are starting out with e-cigarettes and then going on to smoke conventional cigarettes."
• The truth is that the study we relied upon did not measure the time course of electronic cigarette and cigarette use. Thus, it could not determine whether the kids who were using both cigarettes and electronic cigarettes had initiated with smoking or with electronic cigarettes.
• The only study to examine this question found that e-cigarettes are not a gateway to smoking.
• There is no evidence at the current time that kids are starting out with e-cigarettes and then going on to smoke conventional cigarettes.
Placement:
1. Medscape - where the original interview with Dr. Frieden appears
2. The 52 media outlets that carried the story and quoted Dr. Frieden as stating that electronic cigarettes are "condemning many kids to struggling with a lifelong addiction to nicotine."
3. CDC web site
For the Mayo Clinic:
The Rest of the Story has ruled that the Mayo Clinic has lied to the American public by telling them that absolutely no studies have examined the health effects of electronic cigarettes and that doctors have no way of assessing the impact of this product, and has ordered the Mayo Clinic to make this statement. Here is the truth:
• We lied to you when we told you that "No studies have been done to examine the safety of e-cigarettes."
• The truth is that there are at least 10 published studies that examined the health effects of electronic cigarettes. And this doesn't even include the more than 20 studies in which the chemical constituents of electronic cigarette liquids or vapor have been analyzed using gas chromatography/mass spectrometry.
• We also lied to you when we told you that "with nicotine inhalers you receive only nicotine."
• The truth is that nicotine inhalers deliver to users the following chemicals:
Placement:
1. Mayo Clinic web site
2. Mayo Clinic Proceedings
For Stan Glantz:
The Rest of the Story has ruled that I lied to the American public by telling them that studies have demonstrated electronic cigarette experimentation leads to nicotine addiction among nonsmokers who try these products, and has ordered me to make this statement. Here is the truth:
• I lied to you when I told you that in the Choi and Forster study, "e-cigarettes were a pathway to renewed or new nicotine addiction."
• The truth is that the study only measured ever use of electronic cigarettes, not current use, regular use, or addiction to nicotine. Thus, it could not determine whether the kids who had tried electronic cigarettes ever used them again. So it could not tell if these kids were addicted to nicotine. They may have simply tried an electronic cigarette and not vaped again.
• I also lied to you when I told you that my own study demonstrated that electronic cigarettes are "a new route to smoking addiction for adolescents." The study was a cross-sectional one, so I could not draw that conclusion. And I admitted it in the article itself. But that's not what I told you.
Placement:
1. Stan Glantz blog
2. Stan Glantz announcement list
3. UCSF web site
For the University of Kentucky Cancer Center:
The Rest of the Story has ruled that we lied to the American public by telling them that electronic cigarettes are every bit as harmful as smoking, and has ordered us to make this statement. Here is the truth:
• We lied to you when we told you that electronic cigarettes may be "every bit as dangerous" as tobacco cigarettes.
• The truth is that there is abundant evidence that electronic cigarettes are much safer than regular cigarettes. Even the tobacco industry itself acknowledges that smoking is more hazardous than vaping.
Placement:
1. University of Kentucky Cancer Center web site
2. Letter to all Kentucky state legislators
Tuesday, January 14, 2014
In 2014, Rigor of Tobacco Control Science Has Already Declined to a Miniscule Level
We are only two weeks into 2014, but that's all the time needed for the rigor of tobacco control science to have degraded to about the lowest level imaginable.
In a blog commentary entitled "New Evidence that Ecigs Promoting Nicotine Addiction among Young Adults," Stan Glantz argues on his blog that a new study has provided evidence that electronic cigarette use leads to nicotine addiction among young adults who have quit smoking in the past or never smoked in the first place.
Stan writes: "Kelvin Choi and Jean Forester just published a well-done longitudinal study of young adults that followed young adults in Minnesota for one year and examined how attitudes about e-cigarettes affected behavior. They report that one year after entering the study 7.4% of the young adults reported ever using e-cigarettes (21.6% among baseline current smokers, 11.9% among baseline former smokers, and 2.9% among baseline nonsmokers). Put another way, 11.9% of people who had quit smoking before the study started were using e-cigarettes at the end as were 2.9% of people who had never smoked. For these people, e-cigarettes were a pathway to renewed or new nicotine addiction."
The Rest of the Story
The rest of the story is that the study actually did not find that 11.9% of the former smokers were addicted to nicotine at follow-up. Nor did it find that 2.9% of the baseline nonsmokers were currently addicted to nicotine.
And to make matters even worse, the study actually did not even find that 11.9% of the former smokers were currently using electronic cigarettes. Nor did it find that 2.9% of the baseline nonsmokers were currently using electronic cigarettes.
What the study found was that 11.9% of the former smokers had ever tried an electronic cigarette in the past year. This means they might have tried an electronic cigarette once and never taken another puff again. It means they may have tried a single puff on an electronic cigarette just to see what it was like.
Similarly, the study found that 2.9% of the baseline nonsmokers had ever tried an electronic cigarette in the past year. It could have been that the respondent took a single puff on an electronic cigarette and never took another puff.
But instead of telling the truth, Dr. Glantz distorts the results (essentially, he just makes up a new study which didn't take place), and has us believe that this study actually measured addiction to electronic cigarettes. In fact, the study didn't even measure regular use of electronic cigarettes. It didn't even measure current use of electronic cigarettes.
I'm sorry but the rigor of our science has degraded to about the equivalent of that of the tobacco industry of the 1980s.
In a blog commentary entitled "New Evidence that Ecigs Promoting Nicotine Addiction among Young Adults," Stan Glantz argues on his blog that a new study has provided evidence that electronic cigarette use leads to nicotine addiction among young adults who have quit smoking in the past or never smoked in the first place.
Stan writes: "Kelvin Choi and Jean Forester just published a well-done longitudinal study of young adults that followed young adults in Minnesota for one year and examined how attitudes about e-cigarettes affected behavior. They report that one year after entering the study 7.4% of the young adults reported ever using e-cigarettes (21.6% among baseline current smokers, 11.9% among baseline former smokers, and 2.9% among baseline nonsmokers). Put another way, 11.9% of people who had quit smoking before the study started were using e-cigarettes at the end as were 2.9% of people who had never smoked. For these people, e-cigarettes were a pathway to renewed or new nicotine addiction."
The Rest of the Story
The rest of the story is that the study actually did not find that 11.9% of the former smokers were addicted to nicotine at follow-up. Nor did it find that 2.9% of the baseline nonsmokers were currently addicted to nicotine.
And to make matters even worse, the study actually did not even find that 11.9% of the former smokers were currently using electronic cigarettes. Nor did it find that 2.9% of the baseline nonsmokers were currently using electronic cigarettes.
What the study found was that 11.9% of the former smokers had ever tried an electronic cigarette in the past year. This means they might have tried an electronic cigarette once and never taken another puff again. It means they may have tried a single puff on an electronic cigarette just to see what it was like.
Similarly, the study found that 2.9% of the baseline nonsmokers had ever tried an electronic cigarette in the past year. It could have been that the respondent took a single puff on an electronic cigarette and never took another puff.
But instead of telling the truth, Dr. Glantz distorts the results (essentially, he just makes up a new study which didn't take place), and has us believe that this study actually measured addiction to electronic cigarettes. In fact, the study didn't even measure regular use of electronic cigarettes. It didn't even measure current use of electronic cigarettes.
I'm sorry but the rigor of our science has degraded to about the equivalent of that of the tobacco industry of the 1980s.
Monday, January 13, 2014
Graphic Warning Labels in the UK Have Had No Demonstrable Effect on Smoking Prevalence
When I saw Stan Glantz's recent post in which he argued that graphic warning labels will reduce smoking by 16%, I decided to write a commentary noting that the actual experience with graphic warning labels in other countries has not demonstrated any effect, much less a 16% effect. I just noticed, however, that Christopher Snowdon has written the post for me. His excellent commentary demonstrates that the graphic warning label intervention in the UK has not been associated with any significant decline in smoking prevalence.
I do agree with Stan that workplace smoking policies and anti-smoking media campaigns are effective and much needed interventions. However, I do not agree that the scientific evidence supports the conclusion that graphic warning labels will reduce smoking rates by 16%.
I do agree with Stan that workplace smoking policies and anti-smoking media campaigns are effective and much needed interventions. However, I do not agree that the scientific evidence supports the conclusion that graphic warning labels will reduce smoking rates by 16%.
50 Years of Progress Since 1964 Surgeon General's Report? Veteran Anti-Smoking Activist Says Not Exactly
While most of the national tobacco control organizations are boasting about the amazing progress since the 1964 Surgeon General's report on smoking - progress that they claim has continued to this day - one veteran anti-smoking activist is challenging this dogma, arguing that in recent years, the tobacco control movement has squandered the opporunity to reduce smoking-related disease and death. Instead of continued progress, he says, the tobacco control movement has largely been co-opted by a bureaucracy of national organizations that seem more concerned about bolstering their funding streams than fighting the tobacco industry.
This Saturday, on the 50th anniversary of the 1964 report, Dr. Alan Blum - director of the Center for the Study of Tobacco and Society at the University of Alabama - released a new documentary that highlights what he calls "the persistent foot-dragging, fear, and squandering of funds by public health agencies, universities, and medical associations alike in ending the smoking pandemic."
Instead of being a time to celebrate our continued progress in fighting Big Tobacco, Dr. Blum suggests that both the government and the national tobacco control organizations have largely abandoned the fight against the tobacco industry and smoking and instead, have dedicated themselves to funding or seeking funding for research that makes no further contribution to the protection of the public's health.
This Saturday, on the 50th anniversary of the 1964 report, Dr. Alan Blum - director of the Center for the Study of Tobacco and Society at the University of Alabama - released a new documentary that highlights what he calls "the persistent foot-dragging, fear, and squandering of funds by public health agencies, universities, and medical associations alike in ending the smoking pandemic."
Instead of being a time to celebrate our continued progress in fighting Big Tobacco, Dr. Blum suggests that both the government and the national tobacco control organizations have largely abandoned the fight against the tobacco industry and smoking and instead, have dedicated themselves to funding or seeking funding for research that makes no further contribution to the protection of the public's health.
According to a press release accompanying the documentary, Dr. Blum states: "Dr. Terry's indictment of cigarettes should
have marked the beginning of the end of the Marlboro Man. Yet far from
riding off into the sunset, the tobacco industry is riding high in the
saddle. The
50th anniversary of the Surgeon General's report should be a sober
reminder of missed opportunities to curtail cigarette smoking, which
remains the nation's number one avoidable cause of cancer, heart
disease, emphysema, and high health costs. When nearly all government
funding to fight smoking is spent on research that adds little to what
we knew in 1964. It suggests that the most addictive thing about tobacco
is money."
Pointing out that nearly as many Americans smoke today as 50 years ago, Dr. Blum presents a critical yet essential perspective on the current state of the tobacco control movement. He provides multiple examples of how the movement has recently squandered opportunities to reduce smoking-related morbidity and mortality:
- In 1998, the state Attorneys General abandoned their lawsuits against Big Tobacco, essentially being bought off by the tobacco companies. The signing of the Master Settlement Agreement was motivated by the desire for political gain for the Attorneys General and money for the states. Furthermore, between 1998 and 2013, the states have squandered the money, spending only 4% on smoking prevention and cessation.
- In 2009, the Congress enacted legislation that gave the FDA limited regulatory authority over cigarettes. However, the FDA is ill-equipped to regulate a deadly product, has limited ability to do anything that would actually make a dent in cigarette consumption, and to add insult to injury, the tobacco companies can now claim that they are concerned, socially responsible companies that are contributing to the protection of the public's health. They can say, with honesty, that their products are approved by the FDA and that they comply with "stringent" federal regulations intended to protect the public's health.
At the end of the day, Dr. Blum argues, we don't need more research. What we need is action. But tobacco control organizations have become addicted to money and the movement's actions are designed to promote funding streams to these groups rather than to attempt to end the tobacco epidemic.
Dr. Blum's documentary - Blowing Smoke: The Lost Legacy of the Surgeon General's Report - should be required viewing for every tobacco control practitioner.
Friday, January 10, 2014
Why Fiore's Failure to Disclose Conflicts of Interest is So Important
Yesterday, I noted that this month's issue of JAMA features a commentary
co-authored by Dr. Michael Fiore (from the
University of Wisconsin School of Medicine and Public Health) which
reviews the history of tobacco control in the 50 years since the release
of the 1964 Surgeon General's report. Although the article discloses no conflicts of interest, I revealed that Dr. Fiore has a long and intensive history of financial conflicts of interest with the very pharmaceutical companies that manufacture smoking cessation drugs, which he recommends, in the article, be prescribed to every patient who smokes.
Today, I discuss the reasons why hiding a conflict of interest like this is problematic.
The Rest of the Story
There are four major reasons why hiding conflicts of interest are problematic:
1. It Violates Public Health Ethics and Could Be Damaging to the Entire Field of Tobacco Control
One of the basic ethical principles of public health is transparency. It is our responsibility to be forthright with the public about the basis of our opinions about public policy, not to merely express our support or opposition for those policies.
The core ethical principle of transparency was spelled out in a Tobacco Control article (see Fox BJ. Framing tobacco control efforts within an ethical context. Tobacco Control 2005;14[Suppl II]:ii38-ii44).
Fox writes: "The tobacco control community should strive for transparency in its dealings. If the tobacco control community fails to explain its dealings within an appropriate framework, it may be perceived as biased or hiding relationships, and it could lose its reputation for independence."
Thus, not only is hiding conflicts of interest an ethical violation, but it is potentially damaging as well. Once researchers in a field are viewed by the public as hiding relationships, the reputation of the entire field may be tarnished. Just look at what happened to the field of global climate change after it was revealed that merely one of hundreds of researchers in the field may have been biased in his approach.
In addition, hiding conflicts of interest deprives the public (and other researchers) to properly evaluate the validity of one's work. Certainly, one has a different view of the validity of the arguments in Fiore's piece once one becomes aware of his long history of financial relationships with Big Pharma. It is unfair to readers to deprive them of this relevant information. Plus, it is unfair to the journal, because the image of the journal itself could become tarnished if it becomes known that an author hid relevant financial conflicts from readers.
2. It Degrades the Research Integrity of Tobacco Control
One of the features that separates tobacco control research from research conducting historically by the tobacco companies is the integrity of our work. We want and need the public to view the integrity of tobacco control research as being higher than that of work which in the past was conducted by the tobacco companies. If it comes down to tobacco control researchers arguing that secondhand smoke is harmful and tobacco industry-funded studies suggesting that secondhand smoke is not harmful, we want the public to believe us. That requires that the public view our research integrity as being greater than that of the industry.
Previously, there was a significant history of tobacco-funded researchers failing to disclose their conflicts of interest. By now doing the same thing, we are blurring the distinction. Now, the public is going to question the integrity of our research, not just that conducted by or supported by the tobacco companies.
3. It Makes Us Hypocrites When We Criticize Failed Tobacco Industry Disclosures
Tobacco control advocates have often criticized scientists who were supported by the tobacco industry for failing to disclose their funding or other conflicts of interest, such as being paid to author commentaries critical of tobacco control policies. And rightly so. However, if we now engage in the very same tactics, then we become hypocrites, and our credibility in criticizing tobacco industry "hacks" is shot. We don't have any credibility in attacking "tobacco hacks" if we are "Big Pharma hacks."
4. It Hides the Influence of Big Pharma Money on the Field of Tobacco Control and Hinders Smoking Cessation Efforts
Ironically, in the long run, hiding the influence of Big Pharma on smoking cessation policy does not advance the cessation field, but brings it to a grinding halt. The public, and tobacco control practitioners themselves, need to understand the deeply ingrained roots of Big Pharma within the tobacco control movement, especially in the smoking cessation field. Failure to do so will lead to blind following of an industry-based agenda. This is precisely what has happened in tobacco control.
Thanks to deception like that we see here from Dr. Fiore, there is a perception that the use of smoking cessation drugs is the "standard of care." This is far from the truth. If the public, and tobacco practitioners themselves, understood the depth of the connection between those who crafted the "standard of care" (i.e., the Clinical Practice Guideline recommendations) and the industry that manufactures the drugs that are recommended in the Guideline, it would become apparent that these recommendations are heavily biased, not objective, and inappropriate.
Because of the importance of this issue, I have written to the editorial staff of JAMA, urging them to publish a corrective statement, requiring Dr. Fiore to disclose his long and intensive history of conflicts of interest with pharmaceutical companies that manufacture smoking cessation drugs.
Today, I discuss the reasons why hiding a conflict of interest like this is problematic.
The Rest of the Story
There are four major reasons why hiding conflicts of interest are problematic:
1. It Violates Public Health Ethics and Could Be Damaging to the Entire Field of Tobacco Control
One of the basic ethical principles of public health is transparency. It is our responsibility to be forthright with the public about the basis of our opinions about public policy, not to merely express our support or opposition for those policies.
The core ethical principle of transparency was spelled out in a Tobacco Control article (see Fox BJ. Framing tobacco control efforts within an ethical context. Tobacco Control 2005;14[Suppl II]:ii38-ii44).
Fox writes: "The tobacco control community should strive for transparency in its dealings. If the tobacco control community fails to explain its dealings within an appropriate framework, it may be perceived as biased or hiding relationships, and it could lose its reputation for independence."
Thus, not only is hiding conflicts of interest an ethical violation, but it is potentially damaging as well. Once researchers in a field are viewed by the public as hiding relationships, the reputation of the entire field may be tarnished. Just look at what happened to the field of global climate change after it was revealed that merely one of hundreds of researchers in the field may have been biased in his approach.
In addition, hiding conflicts of interest deprives the public (and other researchers) to properly evaluate the validity of one's work. Certainly, one has a different view of the validity of the arguments in Fiore's piece once one becomes aware of his long history of financial relationships with Big Pharma. It is unfair to readers to deprive them of this relevant information. Plus, it is unfair to the journal, because the image of the journal itself could become tarnished if it becomes known that an author hid relevant financial conflicts from readers.
2. It Degrades the Research Integrity of Tobacco Control
One of the features that separates tobacco control research from research conducting historically by the tobacco companies is the integrity of our work. We want and need the public to view the integrity of tobacco control research as being higher than that of work which in the past was conducted by the tobacco companies. If it comes down to tobacco control researchers arguing that secondhand smoke is harmful and tobacco industry-funded studies suggesting that secondhand smoke is not harmful, we want the public to believe us. That requires that the public view our research integrity as being greater than that of the industry.
Previously, there was a significant history of tobacco-funded researchers failing to disclose their conflicts of interest. By now doing the same thing, we are blurring the distinction. Now, the public is going to question the integrity of our research, not just that conducted by or supported by the tobacco companies.
3. It Makes Us Hypocrites When We Criticize Failed Tobacco Industry Disclosures
Tobacco control advocates have often criticized scientists who were supported by the tobacco industry for failing to disclose their funding or other conflicts of interest, such as being paid to author commentaries critical of tobacco control policies. And rightly so. However, if we now engage in the very same tactics, then we become hypocrites, and our credibility in criticizing tobacco industry "hacks" is shot. We don't have any credibility in attacking "tobacco hacks" if we are "Big Pharma hacks."
4. It Hides the Influence of Big Pharma Money on the Field of Tobacco Control and Hinders Smoking Cessation Efforts
Ironically, in the long run, hiding the influence of Big Pharma on smoking cessation policy does not advance the cessation field, but brings it to a grinding halt. The public, and tobacco control practitioners themselves, need to understand the deeply ingrained roots of Big Pharma within the tobacco control movement, especially in the smoking cessation field. Failure to do so will lead to blind following of an industry-based agenda. This is precisely what has happened in tobacco control.
Thanks to deception like that we see here from Dr. Fiore, there is a perception that the use of smoking cessation drugs is the "standard of care." This is far from the truth. If the public, and tobacco practitioners themselves, understood the depth of the connection between those who crafted the "standard of care" (i.e., the Clinical Practice Guideline recommendations) and the industry that manufactures the drugs that are recommended in the Guideline, it would become apparent that these recommendations are heavily biased, not objective, and inappropriate.
Because of the importance of this issue, I have written to the editorial staff of JAMA, urging them to publish a corrective statement, requiring Dr. Fiore to disclose his long and intensive history of conflicts of interest with pharmaceutical companies that manufacture smoking cessation drugs.
Thursday, January 09, 2014
Anti-Smoking Researcher Hides Conflict of Interest With Big Pharma
This month's issue of JAMA features a commentary by Drs. Helene Cole (an associate editor) and Michael Fiore (from the University of Wisconsin School of Medicine and Public Health) which reviews the history of tobacco control in the 50 years since the release of the 1964 Surgeon General's report. The article makes recommendations for strategies to further reduce tobacco-related morbidity and mortality. One of these recommendations is that every patient who smokes be treated with medication. The article also argues that treatment with smoking cessation drugs is the "standard of care" for promoting cessation among smokers.
At the end of the article, the authors include their Conflict of Interest Disclosure, which reads: "The authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest and none were reported." Thus, Dr. Fiore is reporting having no conflicts of interest with regards to the subject matter of this commentary (which includes his recommendation that all smoking patients be treated with drugs, which he states is the standard of care).
The Rest of the Story
Readers who see that Dr. Fiore has declared no conflicts of interest might naturally assume that he has no conflicts of interest to report.
Might they not be surprised, then, to discover the truth:
1. According to his own 2008 JAMA article: "In the past 5 years, Dr Fiore reports that he has lectured and consulted for Pfizer and has served as an investigator on research studies at the University of Wisconsin (UW) that were supported by GlaxoSmithKline, Nabi, Pfizer, and sanofi-aventis."
2. According to his own sworn testimony, at the time of his chairing in 2008 of an expert NIH panel to make recommendations about the recommended clinical strategies for promoting smoking cessation, Dr. Fiore received up to $50,000 in annual resources from GlaxoSmithKline to support his educational, research, and policy activities.
3. In 2006, Dr. Fiore acknowledged that "I have done some consulting work for pharmaceutical companies over the years. Over the past five years, my outside consulting work on an annual basis has ranged between about $10,000 and $30,000 or $40,000 per year."
4. In 1998, the University of Wisconsin appointed him to a named chair, made possible by an unrestricted gift to the University from GlaxoWellcome.
5. In the past, "Dr. Fiore has served as a consultant for, given lectures sponsored by, or has conducted research sponsored by Ciba-Geigy, SmithKline Beecham, Lederle Laboratories, McNeil Consumer Products, Elan Pharmaceutical, Pharmacia, and Glaxo Wellcome."
6. Dr. Fiore directs a tobacco research center that received nearly $1 million in funding from makers of quit-smoking medicine in 2004 and $400,000 in 2005.
7. In a recent set of two articles on treatment for smoking cessation published in the Annals of Behavioral Medicine in April 2011 (article 1; article 2), the conflict of interest statement regarding Dr. Fiore acknowledges that: "Over the last 3 years, Michael C. Fiore served as an investigator on research studies at the University of Wisconsin that were funded by Nabi Biopharmaceuticals."
8. In a December 2010 article on treatment for smoking cessation published in the Wisconsin Medical Journal, the conflict of interest statement regarding Dr. Fiore acknowledges that: "Over the last 3 years, Dr Fiore has served as an investigator in research studies at the University of Wisconsin that were funded by Pfizer and Nabi Biopharmaceuticals."
Amazingly, none of these conflicts of interest are reported in the paper and the reader has no way of knowing this long history of financial conflicts of interest with Big Pharma. I imagine that most readers would be shocked to find out about this intense and long history of financial conflict with Big Pharma, given that Dr. Fiore reported no conflicts of interest.
In my opinion, the fact that there are significant conflicts of interest that should have been disclosed is undeniable. Moreover, it is undeniable that these conflicts are relevant to the subject matter of the paper. The article makes the bold and I believe incorrect statement that treatment with drugs is the "standard of care" for smoking cessation. In fact, I believe that there are many methods that physicians appropriate use to promote smoking cessation in their patients, and medication is only one of these methods. Many physicians recommend other approaches, including counseling, hyponosis, 12-step programs, and cold turkey quitting.
Given the controversial nature of the recommendation that treating every smoker with drugs is the "standard of care," I believe that the long and intense history of conflicts of interest with Big Pharma is absolutely relevant to the present article.
In my view, Dr. Fiore's failure to disclose these conflicts suggests that he really does have something to hide. If not, then what is the danger in not being honest and disclosing these conflicts?
For years, we in tobacco control have attacked tobacco industry-funded scientists or researchers who consulted for tobacco companies for not disclosing their conflicts of interest. It it therefore quite unfortunate, and ironic, that tobacco control researchers do not appear to take their own conflicts of interest seriously and that they, too, are hiding these conflicts from the public.
At the end of the article, the authors include their Conflict of Interest Disclosure, which reads: "The authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest and none were reported." Thus, Dr. Fiore is reporting having no conflicts of interest with regards to the subject matter of this commentary (which includes his recommendation that all smoking patients be treated with drugs, which he states is the standard of care).
The Rest of the Story
Readers who see that Dr. Fiore has declared no conflicts of interest might naturally assume that he has no conflicts of interest to report.
Might they not be surprised, then, to discover the truth:
1. According to his own 2008 JAMA article: "In the past 5 years, Dr Fiore reports that he has lectured and consulted for Pfizer and has served as an investigator on research studies at the University of Wisconsin (UW) that were supported by GlaxoSmithKline, Nabi, Pfizer, and sanofi-aventis."
2. According to his own sworn testimony, at the time of his chairing in 2008 of an expert NIH panel to make recommendations about the recommended clinical strategies for promoting smoking cessation, Dr. Fiore received up to $50,000 in annual resources from GlaxoSmithKline to support his educational, research, and policy activities.
3. In 2006, Dr. Fiore acknowledged that "I have done some consulting work for pharmaceutical companies over the years. Over the past five years, my outside consulting work on an annual basis has ranged between about $10,000 and $30,000 or $40,000 per year."
4. In 1998, the University of Wisconsin appointed him to a named chair, made possible by an unrestricted gift to the University from GlaxoWellcome.
5. In the past, "Dr. Fiore has served as a consultant for, given lectures sponsored by, or has conducted research sponsored by Ciba-Geigy, SmithKline Beecham, Lederle Laboratories, McNeil Consumer Products, Elan Pharmaceutical, Pharmacia, and Glaxo Wellcome."
6. Dr. Fiore directs a tobacco research center that received nearly $1 million in funding from makers of quit-smoking medicine in 2004 and $400,000 in 2005.
7. In a recent set of two articles on treatment for smoking cessation published in the Annals of Behavioral Medicine in April 2011 (article 1; article 2), the conflict of interest statement regarding Dr. Fiore acknowledges that: "Over the last 3 years, Michael C. Fiore served as an investigator on research studies at the University of Wisconsin that were funded by Nabi Biopharmaceuticals."
8. In a December 2010 article on treatment for smoking cessation published in the Wisconsin Medical Journal, the conflict of interest statement regarding Dr. Fiore acknowledges that: "Over the last 3 years, Dr Fiore has served as an investigator in research studies at the University of Wisconsin that were funded by Pfizer and Nabi Biopharmaceuticals."
Amazingly, none of these conflicts of interest are reported in the paper and the reader has no way of knowing this long history of financial conflicts of interest with Big Pharma. I imagine that most readers would be shocked to find out about this intense and long history of financial conflict with Big Pharma, given that Dr. Fiore reported no conflicts of interest.
In my opinion, the fact that there are significant conflicts of interest that should have been disclosed is undeniable. Moreover, it is undeniable that these conflicts are relevant to the subject matter of the paper. The article makes the bold and I believe incorrect statement that treatment with drugs is the "standard of care" for smoking cessation. In fact, I believe that there are many methods that physicians appropriate use to promote smoking cessation in their patients, and medication is only one of these methods. Many physicians recommend other approaches, including counseling, hyponosis, 12-step programs, and cold turkey quitting.
Given the controversial nature of the recommendation that treating every smoker with drugs is the "standard of care," I believe that the long and intense history of conflicts of interest with Big Pharma is absolutely relevant to the present article.
In my view, Dr. Fiore's failure to disclose these conflicts suggests that he really does have something to hide. If not, then what is the danger in not being honest and disclosing these conflicts?
For years, we in tobacco control have attacked tobacco industry-funded scientists or researchers who consulted for tobacco companies for not disclosing their conflicts of interest. It it therefore quite unfortunate, and ironic, that tobacco control researchers do not appear to take their own conflicts of interest seriously and that they, too, are hiding these conflicts from the public.
Wednesday, January 08, 2014
American Lung Association Massively Deceiving the Public in National Electronic Cigarette Op-Ed Piece
Monday's CNN Opinion page featured an op-ed on electronic cigarettes from Harold Wimmer, the president and CEO of the American Lung Association. In the piece, Wimmer argues that Big Tobacco companies are using electronic cigarettes to create "new nicotine addicts" and that they are enticing youth with flavors such as bubble gum and cotton candy.
According to the American Lung Association piece: "Big Tobacco desperately needs new nicotine addicts and is up to its old tricks to make sure it gets them. E-cigarettes are being aggressively marketed to children with flavors like Bazooka Bubble Gum, Cap'n Crunch and Cotton Candy. Joe Camel was killed in the 1990s, but cartoon characters are back promoting e-cigarettes."
Wimmer implies that electronic cigarettes contain tobacco, arguing that: "There is no safe form of tobacco. Right now, the public health and medical community or consumers have no way of knowing what chemicals are contained in an e-cigarette or what the short and long term health implications might be."
Finally, Wimmer implies that the tobacco companies are promoting electronic cigarettes as being safe: "In the absence of meaningful oversight, the tobacco industry has free rein to promote their products as "safe" without any proof." [link is from the original]
The Rest of the Story
Sadly, the American Lung Association is massively deceiving the public, if not outright lying.
There are three blatantly misleading, if not untruthful assertions in the piece:
1. Big Tobacco companies are enticing youth with flavors such as bubble gum and cotton candy.
The Lie: Wimmer implies that Big Tobacco is enticing youth with three specific candy flavors: Bazooka Bubble Gum, Cap'n Crunch, and Cotton Candy.
The Truth: None of the three tobacco companies which market electronic cigarettes in the U.S. are selling electronic cigarettes with bubble gum, cap'n crunch, or cotton candy flavors. In fact, the disposable electronic cigarettes being sold by Big Tobacco companies (i.e., the ones most likely to be purchased by youth) are available solely in classic tobacco or menthol flavors.
Lorillard actually made a decision not to make its disposable electronic cigarettes available in the candy flavors that Blu had been selling prior to Lorillard's acquisition of Blu. Far from demonstrating that tobacco companies are trying to create "new" nicotine addicts, the evidence suggests that Big Tobacco companies are carefully trying to avoid youth customers. They realize that high levels of electronic cigarette use among youth will lead to a quick demise to their business from this innovative product.
At any rate, it is demonstrably false that Big Tobacco is enticing youth with flavors like Bubble Gum, Cap'n Crunch, and Cotton Candy.
2. Electronic cigarettes are a form of tobacco.
The Lie: Wimmer implies that electronic cigarettes are a form of tobacco, emphasizing that there is no form of tobacco and that consumers have no way of knowing what is contained in the electronic cigarette.
The Truth: Electronic cigarettes do not contain or deliver tobacco.
Moreover, the ingredients of electronic cigarettes are well known. Even the components of electronic cigarette vapor have been well characterized. In fact, we know a lot more about the components of electronic cigarette vapor than we do about those of cigarette smoke.
At any rate, it is demonstrably false that electronic cigarettes are a form of tobacco.
3. Tobacco companies are promoting electronic cigarettes as being safe.
The Lie: Wimmer implies that the tobacco companies are promoting electronic cigarettes as being safe, and he links to one electronic cigarette company web site (NEwhere) as support for this statement.
The Truth: None of the cigarette companies have claimed that electronic cigarettes are safe. Moreover, the company which Wimmer cites as evidence of his assertion is not a tobacco company at all. NEwhere is purely an electronic cigarette company. It is not owned by Big Tobacco or any other tobacco company.
Furthermore, the web site to which Wimmer links (NEwhere) does not claim that electronic cigarettes are safe. Instead, it suggests that they are safer than cigarettes. In fact, NEwhere acknowledges that electronic cigarettes are not 100% safe, as they do deliver formaldehyde. It tells its customers that: "electronic cigarettes are not a panacea for smokers. Electronic cigarettes do still contain the harmful chemical formaldehyde in their vapors."
NEwhere also cites a tobacco researcher, a fellow named Michael Siegel, as stating that: "the levels of exposure of E Cigs are either 'well below that of cigarette smoking' in those chemicals that are present, or, more generally electronic cigarette use 'reduces the user's exposure to a wide range of chemicals in tobacco smoke.'" Thus, NEwhere is not stating that electronic cigarettes are absolutely safe, only that they are less hazardous than tobacco cigarettes.
At any rate, it is demonstrably false that any U.S. tobacco company is promoting electronic cigarettes as being safe.
The Truth
Sadly, the truth is that the one lying to and deceiving the public is the American Lung Association. Most electronic cigarette companies are honestly and correctly informing their customers that these products are safer than cigarettes and that they may be helpful to some people in getting them off tobacco cigarettes. These are demonstrably truthful statements.
In contrast, it is the American Lung Association which is lying by implying to the public that Big Tobacco companies are enticing youth with candy-flavored electronic cigarettes such as bubble gum and cotton candy, that electronic cigarettes are a form of tobacco, and that tobacco companies are claiming that electronic cigarettes are safe.
By the way, I agree with Wimmer's ultimate conclusion: that commonsense regulation of electronic cigarettes by the FDA is urgently needed. However, I don't need to lie or deceive the public in order to make that point.
According to the American Lung Association piece: "Big Tobacco desperately needs new nicotine addicts and is up to its old tricks to make sure it gets them. E-cigarettes are being aggressively marketed to children with flavors like Bazooka Bubble Gum, Cap'n Crunch and Cotton Candy. Joe Camel was killed in the 1990s, but cartoon characters are back promoting e-cigarettes."
Wimmer implies that electronic cigarettes contain tobacco, arguing that: "There is no safe form of tobacco. Right now, the public health and medical community or consumers have no way of knowing what chemicals are contained in an e-cigarette or what the short and long term health implications might be."
Finally, Wimmer implies that the tobacco companies are promoting electronic cigarettes as being safe: "In the absence of meaningful oversight, the tobacco industry has free rein to promote their products as "safe" without any proof." [link is from the original]
The Rest of the Story
Sadly, the American Lung Association is massively deceiving the public, if not outright lying.
There are three blatantly misleading, if not untruthful assertions in the piece:
1. Big Tobacco companies are enticing youth with flavors such as bubble gum and cotton candy.
The Lie: Wimmer implies that Big Tobacco is enticing youth with three specific candy flavors: Bazooka Bubble Gum, Cap'n Crunch, and Cotton Candy.
The Truth: None of the three tobacco companies which market electronic cigarettes in the U.S. are selling electronic cigarettes with bubble gum, cap'n crunch, or cotton candy flavors. In fact, the disposable electronic cigarettes being sold by Big Tobacco companies (i.e., the ones most likely to be purchased by youth) are available solely in classic tobacco or menthol flavors.
Lorillard actually made a decision not to make its disposable electronic cigarettes available in the candy flavors that Blu had been selling prior to Lorillard's acquisition of Blu. Far from demonstrating that tobacco companies are trying to create "new" nicotine addicts, the evidence suggests that Big Tobacco companies are carefully trying to avoid youth customers. They realize that high levels of electronic cigarette use among youth will lead to a quick demise to their business from this innovative product.
At any rate, it is demonstrably false that Big Tobacco is enticing youth with flavors like Bubble Gum, Cap'n Crunch, and Cotton Candy.
2. Electronic cigarettes are a form of tobacco.
The Lie: Wimmer implies that electronic cigarettes are a form of tobacco, emphasizing that there is no form of tobacco and that consumers have no way of knowing what is contained in the electronic cigarette.
The Truth: Electronic cigarettes do not contain or deliver tobacco.
Moreover, the ingredients of electronic cigarettes are well known. Even the components of electronic cigarette vapor have been well characterized. In fact, we know a lot more about the components of electronic cigarette vapor than we do about those of cigarette smoke.
At any rate, it is demonstrably false that electronic cigarettes are a form of tobacco.
3. Tobacco companies are promoting electronic cigarettes as being safe.
The Lie: Wimmer implies that the tobacco companies are promoting electronic cigarettes as being safe, and he links to one electronic cigarette company web site (NEwhere) as support for this statement.
The Truth: None of the cigarette companies have claimed that electronic cigarettes are safe. Moreover, the company which Wimmer cites as evidence of his assertion is not a tobacco company at all. NEwhere is purely an electronic cigarette company. It is not owned by Big Tobacco or any other tobacco company.
Furthermore, the web site to which Wimmer links (NEwhere) does not claim that electronic cigarettes are safe. Instead, it suggests that they are safer than cigarettes. In fact, NEwhere acknowledges that electronic cigarettes are not 100% safe, as they do deliver formaldehyde. It tells its customers that: "electronic cigarettes are not a panacea for smokers. Electronic cigarettes do still contain the harmful chemical formaldehyde in their vapors."
NEwhere also cites a tobacco researcher, a fellow named Michael Siegel, as stating that: "the levels of exposure of E Cigs are either 'well below that of cigarette smoking' in those chemicals that are present, or, more generally electronic cigarette use 'reduces the user's exposure to a wide range of chemicals in tobacco smoke.'" Thus, NEwhere is not stating that electronic cigarettes are absolutely safe, only that they are less hazardous than tobacco cigarettes.
At any rate, it is demonstrably false that any U.S. tobacco company is promoting electronic cigarettes as being safe.
The Truth
Sadly, the truth is that the one lying to and deceiving the public is the American Lung Association. Most electronic cigarette companies are honestly and correctly informing their customers that these products are safer than cigarettes and that they may be helpful to some people in getting them off tobacco cigarettes. These are demonstrably truthful statements.
In contrast, it is the American Lung Association which is lying by implying to the public that Big Tobacco companies are enticing youth with candy-flavored electronic cigarettes such as bubble gum and cotton candy, that electronic cigarettes are a form of tobacco, and that tobacco companies are claiming that electronic cigarettes are safe.
By the way, I agree with Wimmer's ultimate conclusion: that commonsense regulation of electronic cigarettes by the FDA is urgently needed. However, I don't need to lie or deceive the public in order to make that point.
Monday, January 06, 2014
If Electronic Cigarettes are a Gateway to Smoking, then Why Were Youth Smoking Rates at an All-Time Low in 2013?
The Centers for Disease Control and Prevention (CDC) is telling the public that electronic cigarettes are a gateway to youth smoking. The CDC has alarmed the public about a concerning doubling of the use of electronic cigarettes by teenagers from 2011 to 2012. Although I pointed out that most of this use occurred among smokers, the CDC nevertheless concluded that electronic cigarettes are leading to increased smoking rates among youth.
Late last month, the University of Michigan released the results of the 2013 Monitoring the Future survey, a national study of youths in grades 8, 10, and 12. Despite the CDC's sirens about how e-cigarettes are leading to an increase in youth smoking, the data show that youth smoking rates reached a record low in 2013.
As summarized by the Campaign for Tobacco-Free Kids: "overall youth smoking declined significantly in 2013, and smoking rates fell to record lows for all three grades surveyed (grades 8, 10 and 12). This is the third year in a row that this survey has found a significant annual decline in youth smoking, which is highly encouraging after several years in which progress had nearly stalled. For all three grades combined, the percentage of students who reported smoking cigarettes in the past month fell from 10.6 percent in 2012 to 9.6 percent in 2013. Smoking declined from 17.1 to 16.3 percent among 12th graders, from 10.8 to 9.1 percent among 10th graders and from 4.9 to 4.5 percent among 8th graders. The declines were statistically significantly for 10th graders and for all three grades combined."
The Rest of the Story
These results hardly seem consistent with the CDC's statements that electronic cigarette use is causing an alarming increase in youth smoking.
Interestingly, it is also possible that electronic cigarettes could have exactly the opposite effect. It is possible that some youths who might have initiated smoking will instead try electronic cigarettes. Further, it is plausible that after using electronic cigarettes, youth may be much less likely to progress to cigarette smoking because compared to the taste and sensation of vaping, the experience of cigarette smoking will not be appealing.
In fact, many vapers have reported that after switching to electronic cigarettes, they have lost the desire to return to smoking because the taste of tobacco cigarettes is no longer pleasant after having experiencing the flavors of electronic cigarettes. It is possible, then, that electronic cigarettes do not serve as a gateway to tobacco smoking but instead, serve as a sort of barrier to tobacco smoking.
While research is clearly needed to understand the trajectory of youth use of electronic cigarettes, the Monitoring the Future survey data do not support the CDC's conclusion that these products are serving as a gateway to youth smoking.
Let's not forget that spurred on by the CDC's report and alarming public statements, politicians have told the public that e-cigarettes are causing youth smoking and eventual cigarette addiction and death:
Senator Richard Blumenthal stated that: ""tobacco companies are using the same despicable tactics with e-cigarettes that they used in previous decades with traditional cigarettes to lure youth down a path of nicotine addiction and eventual death."
Senator Dick Durbin stated that: "the use of e-cigarettes among our nation's kids is ... closely linked to the deadly use of cigarettes."
Senator Ed Markey stated that: "e-cigarettes are a gateway to tobacco use by children and teens...".
The CDC has done enough damage with its irresponsible and untruthful propaganda about electronic cigarettes. It is time that policy decisions be guided by science rather than politics. And the science is now in. It indicates that youth smoking levels are at record lows, which casts serious doubt on the hypothesis that electronic cigarettes are fueling an alarming increase in youth smoking.
Hopefully, 2014 will mark the return of evidence-based tobacco control practice.
Late last month, the University of Michigan released the results of the 2013 Monitoring the Future survey, a national study of youths in grades 8, 10, and 12. Despite the CDC's sirens about how e-cigarettes are leading to an increase in youth smoking, the data show that youth smoking rates reached a record low in 2013.
As summarized by the Campaign for Tobacco-Free Kids: "overall youth smoking declined significantly in 2013, and smoking rates fell to record lows for all three grades surveyed (grades 8, 10 and 12). This is the third year in a row that this survey has found a significant annual decline in youth smoking, which is highly encouraging after several years in which progress had nearly stalled. For all three grades combined, the percentage of students who reported smoking cigarettes in the past month fell from 10.6 percent in 2012 to 9.6 percent in 2013. Smoking declined from 17.1 to 16.3 percent among 12th graders, from 10.8 to 9.1 percent among 10th graders and from 4.9 to 4.5 percent among 8th graders. The declines were statistically significantly for 10th graders and for all three grades combined."
The Rest of the Story
These results hardly seem consistent with the CDC's statements that electronic cigarette use is causing an alarming increase in youth smoking.
Interestingly, it is also possible that electronic cigarettes could have exactly the opposite effect. It is possible that some youths who might have initiated smoking will instead try electronic cigarettes. Further, it is plausible that after using electronic cigarettes, youth may be much less likely to progress to cigarette smoking because compared to the taste and sensation of vaping, the experience of cigarette smoking will not be appealing.
In fact, many vapers have reported that after switching to electronic cigarettes, they have lost the desire to return to smoking because the taste of tobacco cigarettes is no longer pleasant after having experiencing the flavors of electronic cigarettes. It is possible, then, that electronic cigarettes do not serve as a gateway to tobacco smoking but instead, serve as a sort of barrier to tobacco smoking.
While research is clearly needed to understand the trajectory of youth use of electronic cigarettes, the Monitoring the Future survey data do not support the CDC's conclusion that these products are serving as a gateway to youth smoking.
Let's not forget that spurred on by the CDC's report and alarming public statements, politicians have told the public that e-cigarettes are causing youth smoking and eventual cigarette addiction and death:
Senator Richard Blumenthal stated that: ""tobacco companies are using the same despicable tactics with e-cigarettes that they used in previous decades with traditional cigarettes to lure youth down a path of nicotine addiction and eventual death."
Senator Dick Durbin stated that: "the use of e-cigarettes among our nation's kids is ... closely linked to the deadly use of cigarettes."
Senator Ed Markey stated that: "e-cigarettes are a gateway to tobacco use by children and teens...".
The CDC has done enough damage with its irresponsible and untruthful propaganda about electronic cigarettes. It is time that policy decisions be guided by science rather than politics. And the science is now in. It indicates that youth smoking levels are at record lows, which casts serious doubt on the hypothesis that electronic cigarettes are fueling an alarming increase in youth smoking.
Hopefully, 2014 will mark the return of evidence-based tobacco control practice.
Subscribe to:
Posts (Atom)